Immunosuppression Reduction after Diagnosis of Sustained BK Viremia and the Risk of Allograft Rejection, Allograft Loss and Mortality
1Department of Medicine, Western University, London Health Sciences Centre, London, ON, Canada, 2Epidemiology and Biostatistics, Western University, London, ON, Canada, 3Department of Medicine, University Of Toronto, University Health Network, Toronto, ON, Canada
Meeting: 2019 American Transplant Congress
Abstract number: C251
Keywords: Immunosuppression, Kidney, Polyma virus, Rejection
Session Information
Session Name: Poster Session C: Kidney: Polyoma
Session Type: Poster Session
Date: Monday, June 3, 2019
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:00pm-7:00pm
Presentation Time: 6:00pm-7:00pm
Location: Hall C & D
*Purpose: BK viremia increases the risk of allograft loss after renal transplantation. Current guidelines recommend immunosuppression reduction (IsR) after the diagnosis of BK viremia. The aim of our study was to demonstrate the risk of graft rejection, graft loss, and death after IsR considering baseline immunologic risk.
*Methods: BKV screening included plasma BKV-PCR (RealStar® BKV PCR, Altona Diagnostics, Kit 1.2 assay) every 1-3 months in the first 2 years after transplantation. In case of sustained BK viremia (i.e., ≥2 consecutive BKV positive plasma samples spanning ≥ 3 weeks), we regularly reduced the dose of mycophenolate mofetil while targeting tacrolimus serum trough level <6 ng/ml. We monitored BK viral load and allograft function for two years. Univariate and multivariable logistic regression analyses - with Poisson family and log link - were used to report crude and adjusted risk ratios (ARR), respectively. Covariates with a p-value less than 0.15 in crude model were entered into multivariable model.
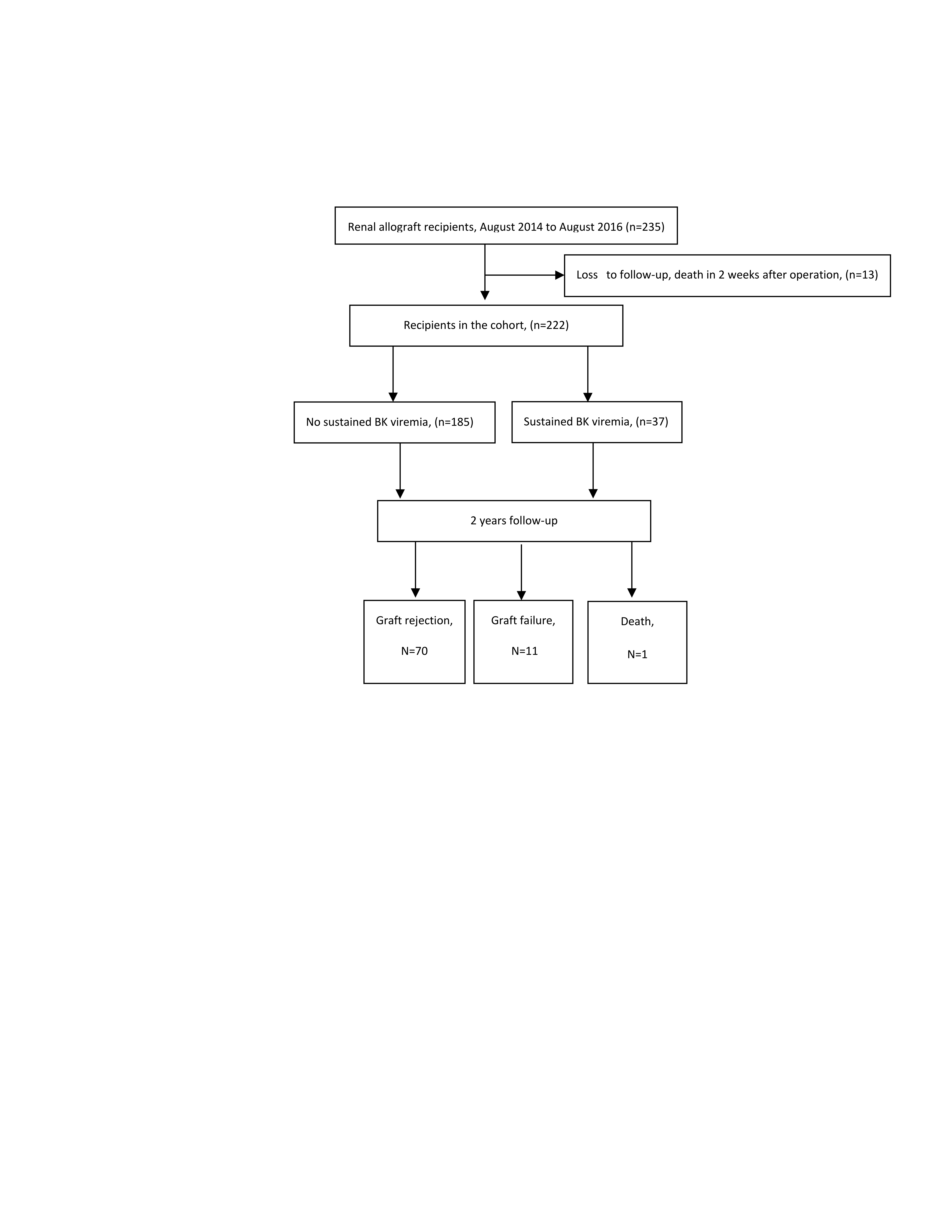
*Results: 37 recipients (16.7%) developed sustained BK viremia (median 66, IQR: 48-121 days after transplantation). Graph 1 shows the flowchart of study in detail. Median viral load at the time of IsR was 19,600 (IQR: 1,200-3,380,000) copies/ml. 94.6% of patients achieved BKV nadir (viral load <500 copies/ml) after IsR. Recipients with sustained BK viremia requiring IsR were 2.44 (1.71, 3.48) times more likely to develop acute rejection. In multivariable regression model, we controlled the effects of following confounders: donor-specific antibodies (DSA), highly sensitization and/or ABO incompatibility. In this analysis, IsR significantly increased the risk of rejection (ARR: 2.43; CI95%:1.72-3.45). However, allograft rejection after IsR was commonly mild, with 74% of cases compatible with borderline rejection by Banff criteria. Allograft function improved in 47% of patients with borderline rejection without treatment of rejection. 2-year risk of allograft failure (5.6% vs 4.9%, p=0.867) and death (0 vs 0.5%, p=0.657) did not considerably increase after IsR. Age, sex, cold ischemia time, donor status (living vs deceased), CMV serostatus, delayed graft function, induction and maintenance immunosuppression did not increase the risk of rejection. High degree of sensitization (ARR: 1.87; CI95%:1.14- 3.07) and detectable DSA (ARR: 1.53; CI95%: 0.92- 2.52) also increased the risk of allograft rejection.
*Conclusions: IsR following the diagnosis of sustained BK viremia significantly increases the risk of allograft rejection however rejection is frequently borderline and may not require treatment. IsR does not seem to be associated with allograft loss or mortality.
To cite this abstract in AMA style:
Dhufairi FAAl, Shokoohi M, Jevnikar AM, House AA, Kumar D, Hosseini-Moghaddam SM. Immunosuppression Reduction after Diagnosis of Sustained BK Viremia and the Risk of Allograft Rejection, Allograft Loss and Mortality [abstract]. Am J Transplant. 2019; 19 (suppl 3). https://atcmeetingabstracts.com/abstract/immunosuppression-reduction-after-diagnosis-of-sustained-bk-viremia-and-the-risk-of-allograft-rejection-allograft-loss-and-mortality/. Accessed April 4, 2026.« Back to 2019 American Transplant Congress