“I'll Be Back”: Increasing Readmission Rates in the Era of the New Kidney Allocation System
MUSC, Charleston.
Meeting: 2018 American Transplant Congress
Abstract number: B84
Keywords: Allocation, Kidney, Kidney transplantation, Risk factors
Session Information
Session Name: Poster Session B: Kidney Deceased Donor Allocation
Session Type: Poster Session
Date: Sunday, June 3, 2018
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:00pm-7:00pm
Presentation Time: 6:00pm-7:00pm
Location: Hall 4EF
Background: National analysis of the impact of the new KAS has indicated an increase in DGF rates, total inpatient hospital costs & 30 day readmission rates. We observed a significant increase in our readmissions post-KAS implementation. The aim of this study was to evaluate readmission etiology pre & post-KAS to facilitate targeted interventions.
Methods: This was a 13-yr longitudinal cohort study of adult KTX recipients transplanted between 2005-16, f/u thru 2017. Pts were designated pre-KAS if their tx date occurred before Dec 2014. Living donor, peds & multi-organ pts were excluded. All readmissions w/in 1-yr of tx were abstracted from medical records & assigned to 1 of 12 primary etiologies based on dc diagnoses (rejection, infection, GI, surgical, CV, DM, hemodynamics/volume, AKI, ADE, electrolyte, cytopenia & other). Readmission rates were estimated in 100 patient-years (100 pt-yrs) & multivariable generalized linear modeling was used to assess adjusted trends in rates over time; Cox regression was used to assess the adjusted impact of readmission etiology on graft survival.
Results: 1,540 KTX were included (Table 1). Infections (23.7 per 100 pt-yrs) & surgical complications (10.8 per 100 pt-yrs) were the most common reasons for readmission followed by GI (7.3 per 100 pt-yrs) & volume (5.5 per 100 pt-yrs). In the fully adjusted overall readmission analysis, pts in the post-KAS era experienced a 23% higher rate of readmission (IRR 95% CI 1.02-1.48). This greatly varied by etiology: post-KAS pts were significantly more likely to be readmitted for GI issues (1.96, 95% CI 1.30-2.94), surgical complications (1.62, 95% CI 1.15-2.30), DM (1.58, 95% CI 0.95-2.64) and other causes (1.55, 95% CI 1.09-2.20). Readmissions rates for rejection, infection, CV events, hemodynamics, AKI, cytopenias and electrolytes did not significantly differ across KAS eras.
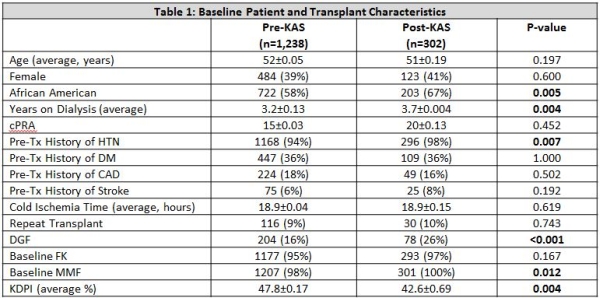
Conclusion: Despite no significant differences in cold ischemia time or KDPI in the post-KAS cohort, DGF rates increased significantly, likely reflecting uncaptured changes in graft quality & potentially contributing to increases in GI readmissions & readmissions for surgical complications.
CITATION INFORMATION: Pilch N., Mardis C., Meadows H., Fleming J., Patel N., Perez C., Baliga P., Dubay D., Rohan V., Rao V., Taber D. “I'll Be Back”: Increasing Readmission Rates in the Era of the New Kidney Allocation System Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Pilch N, Mardis C, Meadows H, Fleming J, Patel N, Perez C, Baliga P, Dubay D, Rohan V, Rao V, Taber D. “I'll Be Back”: Increasing Readmission Rates in the Era of the New Kidney Allocation System [abstract]. https://atcmeetingabstracts.com/abstract/ill-be-back-increasing-readmission-rates-in-the-era-of-the-new-kidney-allocation-system/. Accessed May 18, 2026.« Back to 2018 American Transplant Congress