Geographic Disparities in Access to Deceased Donor Kidney Transplant.
1Scientific Registry of Transplant Recipients, Minneapolis
2Johns Hopkins University, Baltimore
3U.S. Naval Academy, Annapolis
Meeting: 2017 American Transplant Congress
Abstract number: 500
Keywords: Allocation, Kidney, Procurement
Session Information
Session Name: Concurrent Session: Disparities in Kidney Transplantation
Session Type: Concurrent Session
Date: Tuesday, May 2, 2017
Session Time: 4:30pm-6:00pm
 Presentation Time: 5:30pm-5:42pm
Presentation Time: 5:30pm-5:42pm
Location: E451a
In 2015, SRTR was asked by HRSA to investigate geographic disparities in access to deceased donor kidney transplant. To account for the potential impact of the new kidney allocation system (KAS) on access to deceased donor transplant, we analyzed pre- and post-KAS data separately.
We found geographic disparities in many aspects of deceased donor transplant at the donation service area (DSA) level. Variability was substantial in unadjusted deceased donor transplant rates across DSAs, ranging from 4.6 transplants per 100 active patient-years to 87.7 (Figure 1). Adjusted models (described elsewhere) showed similar trends.
To further explain the variation in transplant rates, we examined adjusted transplant rates (demand) and organ procurement organization (OPO) kidney yield (supply) across DSAs. DSAs with a high adjusted supply of kidneys typically had relatively higher adjusted demand that was not met by local supply; i.e. demand outpaced supply in DSAs with high transplant rates. Additionally, low-supply DSAs were more likely to transplant more kidneys than the expected local OPO kidney yield, suggesting that programs in low-supply DSAs are more likely to import kidneys and/or use marginal kidneys in an attempt to meet local demand (Figure 2).
We also found differences across DSAs in the recovery rate per referred in-hospital death and in the waitlisting rate of ESRD patients. These trends were in an opposing direction to the differences in deceased donor transplant rates, which may help explain the disparities in transplant rates.
Finally, we found no major changes pre- or post-KAS. KAS was not designed to reduce geographic disparities in access to transplant, nor is there evidence that it did.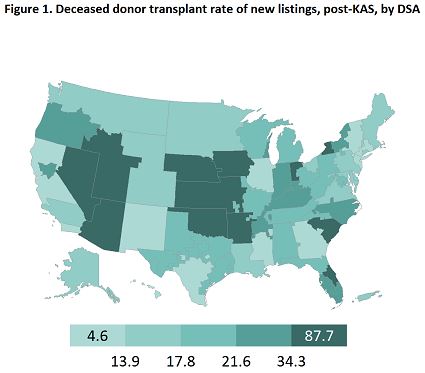

CITATION INFORMATION: Gustafson S, Wey A, Thompson B, Massie A, Zhou S, Salkowski N, Segev D, Gentry S, Snyder J. Geographic Disparities in Access to Deceased Donor Kidney Transplant. Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Gustafson S, Wey A, Thompson B, Massie A, Zhou S, Salkowski N, Segev D, Gentry S, Snyder J. Geographic Disparities in Access to Deceased Donor Kidney Transplant. [abstract]. Am J Transplant. 2017; 17 (suppl 3). https://atcmeetingabstracts.com/abstract/geographic-disparities-in-access-to-deceased-donor-kidney-transplant/. Accessed May 27, 2026.« Back to 2017 American Transplant Congress