Evaluation of Scoring Systems Predicting Patient Survival at Time of Kidney Transplantation.
Nephrology, Charite, Berlin, Germany.
Meeting: 2016 American Transplant Congress
Abstract number: 43
Keywords: Allocation, Morbidity, Mortality, Risk factors
Session Information
Session Name: Concurrent Session: Kidney Transplantation: Outcomes, Matching and Marginal Donors
Session Type: Concurrent Session
Date: Sunday, June 12, 2016
Session Time: 2:30pm-4:00pm
 Presentation Time: 2:54pm-3:06pm
Presentation Time: 2:54pm-3:06pm
Location: Ballroom B
Introduction:Estimating life expectancy in kidney transplant recipients (KTR) at time of transplantation is important to achieve the best functional match between patient and graft survival. Various scores exist assessing life expectancy of patients, however few of them have been validated in KTR.
Methods:This retrospective long-term study included 878 deceased KTR (mean age 54 yrs) transplanted 1998-2014. All relevant co-morbidities were determined at time of transplantation. Estimated-Post-Transplant-Survival (EPTS), Charlson Comorbidity Score (CCI), age-adjusted CCI, Davies Score, Recipient Risk Score (RRS) and Khan Score calculated at time of transplant were evaluated. Survival data were analyzed with time-dependent ROC-curves over maximal 23 years using a Kaplan Meier method. R2-coefficients for censored time-to-event data were implemented. A cox model for each score was established.
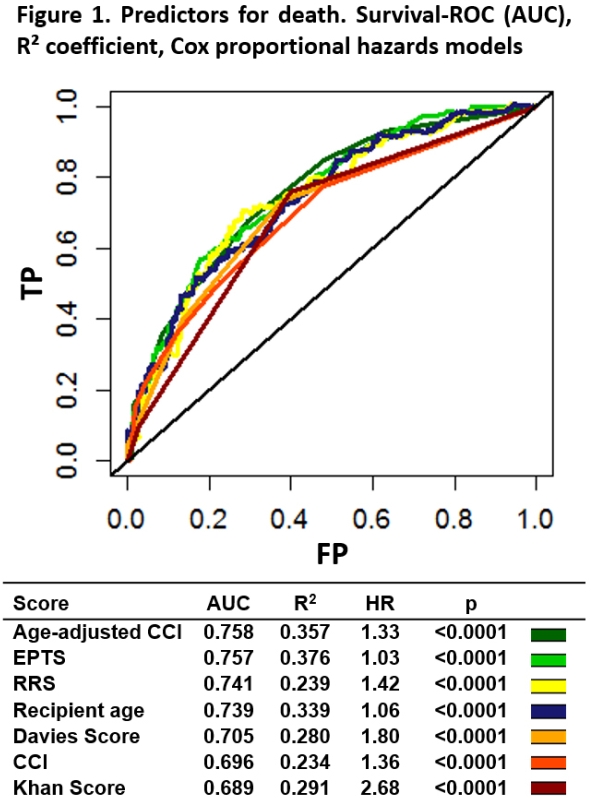
Results:All scores were significantly associated with mortality. Best fit (assessed by R2 coefficient) reached the EPTS (including age, time on dialysis, prior kidney transplantation, diabetes), followed by the age-adjusted CCI (including age, myocardial infarction, congestive heart failure, peripheral vascular disease, dementia, chronic pulmonary disease, connective tissue disease, peptic ulcer disease, liver disease, diabetes, hemiplegia, malignancy, leukemia, lymphoma, AIDS). Age-adjusted CCI and EPTS best predicted mortality in a survival-ROC analysis. The AUC were 0.758 and 0.757. Other scores or age alone did not reach the level of concordance of age-adjusted CCI and EPTS (Fig 1). The age-adjusted CCI reached this predictive value by assessing comorbidity in more detail, despite neglecting important KTR-specific relevant influence factors used in the EPTS.
Discussion:The EPTS (in use in the US-allocation) may be improved including further important comorbid conditions for estimating life expectancy especially in elderly and comorbid KTR. Utilization of a refined scoring for the allocation in these KTR may help to achieve the best functional match with high KDPI kidneys and may also avoid the discard of organs without compromising the outcome.
CITATION INFORMATION: Staeck O, Khadzhynov D, Kleinsteuber A, Lehner L, Duerr M, Budde K, Halleck F. Evaluation of Scoring Systems Predicting Patient Survival at Time of Kidney Transplantation. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Staeck O, Khadzhynov D, Kleinsteuber A, Lehner L, Duerr M, Budde K, Halleck F. Evaluation of Scoring Systems Predicting Patient Survival at Time of Kidney Transplantation. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/evaluation-of-scoring-systems-predicting-patient-survival-at-time-of-kidney-transplantation/. Accessed May 26, 2026.« Back to 2016 American Transplant Congress