Detecting Renal Allograft Inflammation Using Quantitative Urine Metabolomics and CXCL10.
1Internal Medicine, University of Manitoba, Winnipeg, MB, Canada
2Pediatrics & Child Health, University of Manitoba, Winnipeg, MB, Canada
3Biological Sciences, University of Alberta, Edmonton, AB, Canada
4Pathology, University of Manitoba, Winnipeg, MB, Canada.
Meeting: 2016 American Transplant Congress
Abstract number: 133
Keywords: Kidney transplantation, Monitoring, Protocol biopsy, Rejection
Session Information
Session Name: Concurrent Session: Kidney Immune Monitoring 1
Session Type: Concurrent Session
Date: Sunday, June 12, 2016
Session Time: 4:30pm-6:00pm
 Presentation Time: 4:42pm-4:54pm
Presentation Time: 4:42pm-4:54pm
Location: Ballroom C
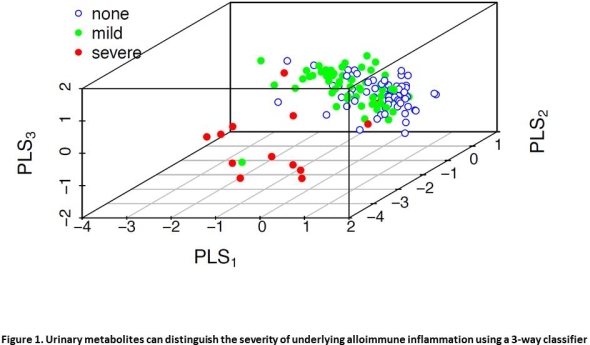
Background. We studied urine metabolomics (UM) alone or combined with urine CXCL10 to non-invasively detect cellular infiltrates in renal allograft biopsies.
Methods. Urines (n=137) were obtained prior to biopsy in 113 patients with no (n=66), mild (borderline or subclinical; n=58) or severe (clinical; n=13) rejection. UM was performed with Direct Flow Injection-Tandem Mass Spectrometry (DFI-MS/MS) using multiple reaction monitoring. Urine CXCL10 was measured by ELISA. UM data was analyzed with PLS-DA, validated with leave-one-out cross-validation, and an optimal two-component model was developed. CXCL10 area under the curve (AUC) was determined and a net reclassification index (NRI) and integrated discrimination index (IDI) analyses were performed.
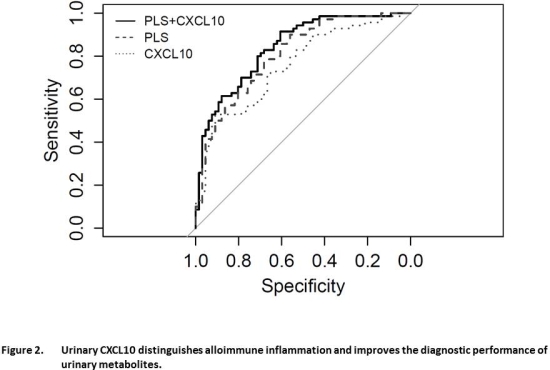
Results. A three-way PLS2 classifier demonstrated that UM discriminated the three groups (Cohen's kappa 0.601, 95%CI 0.46-0.74, p<0.001). UM and CXCL10 demonstrated an AUC 0.81 (95%CI 0.74-0.88) and 0.76 (95%CI 0.68-0.84) respectively; and a combined AUC 0.84 (95%CI 0.78-0.91) for detecting alloimmune inflammation that was improved by NRI and IDI. Urinary CXCL10 was the best discriminator, followed by urine acylcarnitines and hexose.
Conclusions. UM can accurately and non-invasively discriminate non-inflamed biopsies from subclinical and clinical inflammation, and the addition of urine CXCL10 had a modest but significant effect on overall diagnostic performance. These data suggest that UM and CXCL10 may be useful for non-invasive monitoring of alloimmune inflammation in renal transplant patients.
CITATION INFORMATION: Ho J, Sharma A, Mandal R, Wishart D, Wiebe C, Storsley L, Karpinski M, Gibson I, Nickerson P, Rush D. Detecting Renal Allograft Inflammation Using Quantitative Urine Metabolomics and CXCL10. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Ho J, Sharma A, Mandal R, Wishart D, Wiebe C, Storsley L, Karpinski M, Gibson I, Nickerson P, Rush D. Detecting Renal Allograft Inflammation Using Quantitative Urine Metabolomics and CXCL10. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/detecting-renal-allograft-inflammation-using-quantitative-urine-metabolomics-and-cxcl10/. Accessed May 16, 2026.« Back to 2016 American Transplant Congress