Covid Infection Among Kidney Transplant Recipients: Management and Outcomes
Medical University of South Carolina, Charleston, SC
Meeting: 2021 American Transplant Congress
Abstract number: 796
Keywords: Infection, Kidney transplantation
Topic: Clinical Science » Infectious Disease » Kidney Infectious Non-Polyoma & Non-Viral Hepatitis
Session Information
Session Name: Kidney Infectious Non-Polyoma & Non-Viral Hepatitis
Session Type: Poster Abstract
Session Date & Time: None. Available on demand.
Location: Virtual
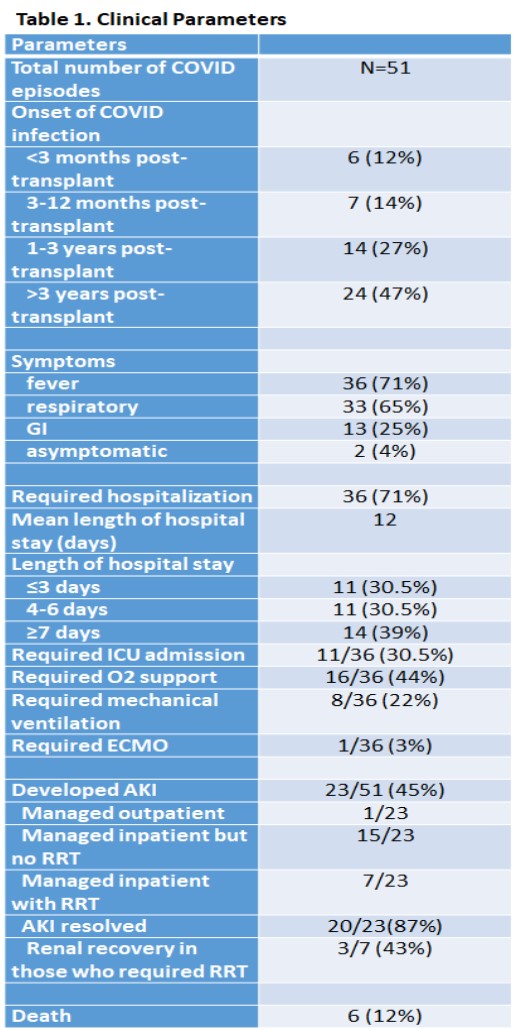
*Purpose: COVID pandemic has posed a significant challenge among kidney transplant recipients (KTR) due to their immunocompromised state. There is uncertainty on immunosuppression management among those who have COVID infection. We sought to better understand the clinical course, management, and outcomes of our KTR who developed COVID infection.
*Methods: Single-center experience of COVID infected KTR. Baseline demographics, clinical data, management, and outcomes were obtained by manual chart abstraction of the EMR.
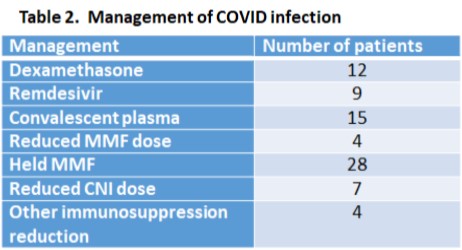
*Results: 50 KTR had COVID infection. Mean age was 53; 50% males; 74% African-Americans. Fever was the most common symptom (71%); 36 patients (71%) required hospitalization; 11 (22%) required ICU admission and 8 (16%) required mechanical ventilation. 23 developed AKI with one-third requiring RRT; 50% of patients requiring RRT eventually had renal recovery. Majority of admitted patients received dexamethasone, remdesivir, and convalescent plasma. In terms of immunosuppression, 28 of 49 (57%) had their MMF held while 8% had MMF dose reductions; one had everolimus held and one had AZA held; 7 (14%) had CNI dose reductions with none held. Six patients (12%) died. Those who died were significantly more likely to receive dexamethasone (42% vs 2%; p=0.002), remdesivir (33% vs 7%; p=0.027), and convalescent plasma (40% vs 0%; p=0.001). Mortality rates were similar across those who had immunosuppressive agents dose reduced vs held vs not adjusted (11% vs 17% vs 12%, respectively; p=0.919). CNI dose reductions tended to be more common in those who died (43% vs 7%; p=0.122). There were no subsequent acute rejections or graft losses in those who recovered.
*Conclusions: KTR represent a vulnerable patient population during COVID. Due to their immunocompromised state and often more severe clinical presentation, the majority require hospitalization, with a significant number needing ICU admission and mechanical ventilation. Severe illness led to higher use of dexamethasone, remdesivir and covalescent plasma in those who ultimately died of COVID. It is unclear what impact immunosuppression dose reductions had on the COVID clinical course, but these reductions did not appear to increase risk of rejection or graft loss.
To cite this abstract in AMA style:
Price A, Soliman K, Zayas C, Rao V, Casey M, Taber D, Salas MPosadas. Covid Infection Among Kidney Transplant Recipients: Management and Outcomes [abstract]. Am J Transplant. 2021; 21 (suppl 3). https://atcmeetingabstracts.com/abstract/covid-infection-among-kidney-transplant-recipients-management-and-outcomes/. Accessed May 15, 2026.« Back to 2021 American Transplant Congress