BK Virus (BKV) Screening Algorithm
Rush University Medical Center, Chicago
Meeting: 2013 American Transplant Congress
Abstract number: A593
Introduction: BKV nephropathy (BKN) can cause allograft loss in renal transplant recipients. BKV surveillance with preemptive intervention has been shown to reduce the incidence of BKN. Surveillance algorithms are not standardized and involve frequent, costly testing. We hypothesize that a negative urine BK PCR early post-transplant is associated with low risk of future BK nephropathy.
Methods: 121 renal transplant recipients are being prospectively studied and 78 patients currently have ≥ 12 months of evaluable data. Urine and plasma BK PCR are performed at 0, 2, 4, 6, and 12 months post-transplant. Transplant providers are blinded to the urine BK PCR results so that treatment strategies are based solely on serum BK viral loads (VL). Clinical data including demographics, renal function, immunosuppression, and biopsy results will be collected for 18 months post-transplant. Significant BK activity is defined as plasma BK VL > 104 copies/mL or urine BK VL > 107 copies/mL.
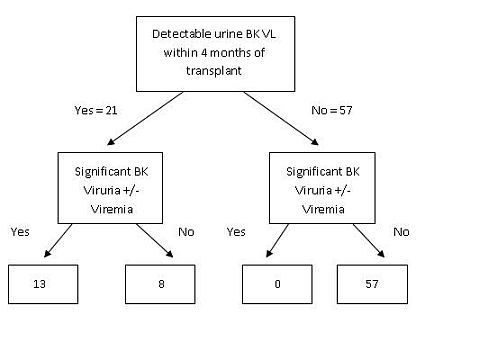
Results: Of 78 patients with 12 months of evaluable data, 57 had no BKV detected in their urine during the first 4 months post-transplant and 21 had BKV detected. None of the 57 went on to develop significant BK activity; 13 of the patients with BK viruria during the first 4 months later developed significant BK activity (p<0.001, Fisher’s exact test). 2 patients developed BKN. Both have poor renal function but have not required renal replacement therapy. 24% (4/13) of patients with and 11% (7/65) of patients without significant BK activity had biopsy-proven rejection (p=0.21, Fisher’s exact test). At 12 months, there was no significant change in renal function among patients with or without significant BK activity (p=0.15, student’s T-test).
Conclusions: Our results suggest that the presence of BK viruria within 4 months of transplant identifies a subgroup of renal transplant patients who are at risk for BKN and require ongoing BK surveillance. Patients without early BK viruria may only need BK testing when there is a decline in renal function or an augmentation of immunosuppression. If confirmed by the completed study, these results may offer a relatively simple and cost effective approach to BKV monitoring after renal transplant.
To cite this abstract in AMA style:
Hodowanec A, Singh K, Stevens J, Crank C, Saltzberg S, Hollinger E, Jensik S, Simon D. BK Virus (BKV) Screening Algorithm [abstract]. Am J Transplant. 2013; 13 (suppl 5). https://atcmeetingabstracts.com/abstract/bk-virus-bkv-screening-algorithm/. Accessed June 3, 2026.« Back to 2013 American Transplant Congress