Association of Transplant Volume and Survival in Pediatric Kidney Transplants
1United Network for Organ Sharing, Richmond, VA
2Baylor Coll Med & Texas Children's Hosp., Houston, TX.
Meeting: 2015 American Transplant Congress
Abstract number: D219
Keywords: Kidney transplantation, Outcome, Pediatric
Session Information
Session Name: Poster Session D: Pediatric Clinical Kidney Transplantation
Session Type: Poster Session
Date: Tuesday, May 5, 2015
Session Time: 5:30pm-6:30pm
 Presentation Time: 5:30pm-6:30pm
Presentation Time: 5:30pm-6:30pm
Location: Exhibit Hall E
Background. Center specific volume has been shown to correlate with outcomes for many procedures in the adult population. The current analysis was conducted to determine the impact of transplant (tx) volume on survival in pediatric (aged <18y) recipients of kidney (KI) tx. The OPTN Pediatric Committee recommended 12 as a minimal tx volume that demonstrated pediatric (ped) training and expertise.
Data and Methods. OPTN data was analyzed for ped KI alone tx during 2000-2010. Tx volume was determined based on the number of KI alone tx during 2000-2010 and used to categorize centers (ctrs) into low (<12 tx) or high (12+ tx) volume. Kaplan-Meier (KM) survival within 5 yrs was estimated among ped KI alone tx and compared between low vs. high volume ctrs using a log-rank test. A multivariable Cox regression was used to determine the association of tx volume and post-tx 5-yr survival. Results of the Cox analysis are presented as a hazard ratio (HR) and p-value, with HR>1 indicating worse survival.
Results. During 2000-2010, 212 tx ctrs that performed a total of 8,339 ped kidney tx were included in the analysis; 92 were low volume ctrs with a total of 272 ped KI tx (3%), and 120 were high volume ctrs with a total of 8,067 ped KI tx (97%). Figure 1 shows a significant difference in KM graft and patient survival between tx performed at low vs. high volume ctrs. 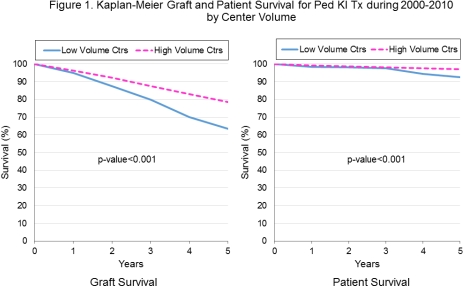
Results of the Cox regression analysis suggested that, after adjusting for other risk factors, tx performed at low volume ctrs, compared to tx performed at high volume ctrs, were associated with both significantly worse 5-yr graft survival (HR=1.3; p=0.01) and 5-yr patient survival (HR=2.0; p<0.01).
Conclusions. As a group, ctrs that performed <12 ped KI tx during 2000-2010 had worse 5-yr graft and patient survival than ctrs that performed 12+ ped KI tx during that period. This finding supports the need to develop minimal experience criteria for physicians and surgeons caring for ped KI tx recipients.
To cite this abstract in AMA style:
Cherikh W, Wilk A, Flavin C, Brewer E. Association of Transplant Volume and Survival in Pediatric Kidney Transplants [abstract]. Am J Transplant. 2015; 15 (suppl 3). https://atcmeetingabstracts.com/abstract/association-of-transplant-volume-and-survival-in-pediatric-kidney-transplants/. Accessed May 29, 2026.« Back to 2015 American Transplant Congress