Adjustment for Race and Ethnicity Does Not Change Transplant Center Outcome Metrics for Liver Recipients
1Emory University, Atlanta, GA, 2University of Miami, Miami, FL
Meeting: 2022 American Transplant Congress
Abstract number: 267
Keywords: African-American, Outcome, Public policy
Topic: Clinical Science » Public Policy » 21 - Non-Organ Specific: Public Policy & Allocation
Session Information
Session Name: Non-Organ Specific: Public Policy & Allocation
Session Type: Rapid Fire Oral Abstract
Date: Monday, June 6, 2022
Session Time: 3:30pm-5:00pm
 Presentation Time: 4:30pm-4:40pm
Presentation Time: 4:30pm-4:40pm
Location: Hynes Room 311
*Purpose: Concerns have been raised about whether transplant center metrics should be adjusted for race and ethnicity given long-standing disparities in outcomes. Proponents of adjustment cite the need to avoid “penalizing” centers who serve racial and ethnic minorities, while critics argue that adjustment obscures potentially remediable disparities. We examined the impact of race and ethnicity adjustment on center performance for liver recipients.
*Methods: Data on adult, single organ, deceased donor liver recipients were obtained from SRTR. We identified two cohorts: transplanted from 07/01/2015 to 12/31/2017 (3-year outcomes) and from 01/01/2018 to 03/12/2020 (1-year outcomes). Our outcome was a composite of death, graft failure, or re-transplantation. Patients were assigned risk scores using two models: 1) SRTR’s current risk adjustment model including race and ethnicity, and 2) same as model 1, without race and ethnicity. Hazard ratios for patient race and ethnicity were obtained by comparing the observed number of outcomes to the expected from model 2 for each group. Hazard ratios for each center were calculated by comparing the observed outcomes to the expected for both models. Fit was assessed for each model using the concordance statistic.
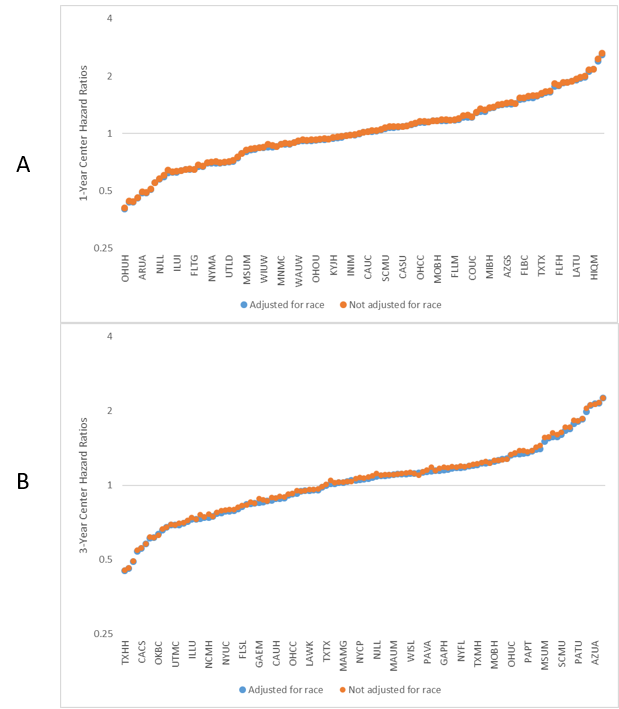
*Results: At 1 year, Asian patients had 14% higher risk of the composite outcome than expected (95% CI: 0.98, 1.30) and non-Hispanic Black patients had 27% higher risk than expected (95% CI: 1.03, 1.51); in contrast, non-Hispanic White patients had similar risk to expected (HR: 0.99, 95% CI: 0.93, 1.06). At 3 years, non-Hispanic Black patients had 40% higher risk of the composite outcome than expected (95% CI: 1.22, 1.58). At 1 year (Figure 1A) and 3 years (Figure 1B), adjustment for race and ethnicity had minimal effect on center hazard ratios. Model fit was equivalent for both models (1-year concordance: 0.80, 3-year: 0.88).
*Conclusions: Adjustment for race and ethnicity should serve the advancement of health equity. Despite persistent disparities in liver transplant outcomes by race and ethnicity, we show that adjustment for these factors has negligible impact on transplant center performance metrics. Future metrics should move away from penalization altogether and focus on measuring and promoting equity.
To cite this abstract in AMA style:
Ross-Driscoll K, Gunasti J, Harding J, Goldberg D, Lynch R, Patzer R. Adjustment for Race and Ethnicity Does Not Change Transplant Center Outcome Metrics for Liver Recipients [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/adjustment-for-race-and-ethnicity-does-not-change-transplant-center-outcome-metrics-for-liver-recipients/. Accessed May 14, 2026.« Back to 2022 American Transplant Congress