A Payer’s Perspective: The Cost of Hemodialysis versus Living Donor Kidney Transplant for Kidney Failure Patients in Nigeria
1University of Toledo College of Medicine and Life Sciences, Toledo, OH, 2Surgical Specialists of Charlotte, Matthews, NC, 3Department of Internal Medicine, Nephrology Unit, Federal Medical Centre, Umuahia, Abia State, Nigeria
Meeting: 2021 American Transplant Congress
Abstract number: 717
Keywords: Economics, Kidney transplantation, Renal failure, Resource utilization
Topic: Clinical Science » Ethics » Non-Organ Specific: Economics & Ethics
Session Information
Session Name: Non-Organ Specific: Economics & Ethics
Session Type: Poster Abstract
Session Date & Time: None. Available on demand.
Location: Virtual
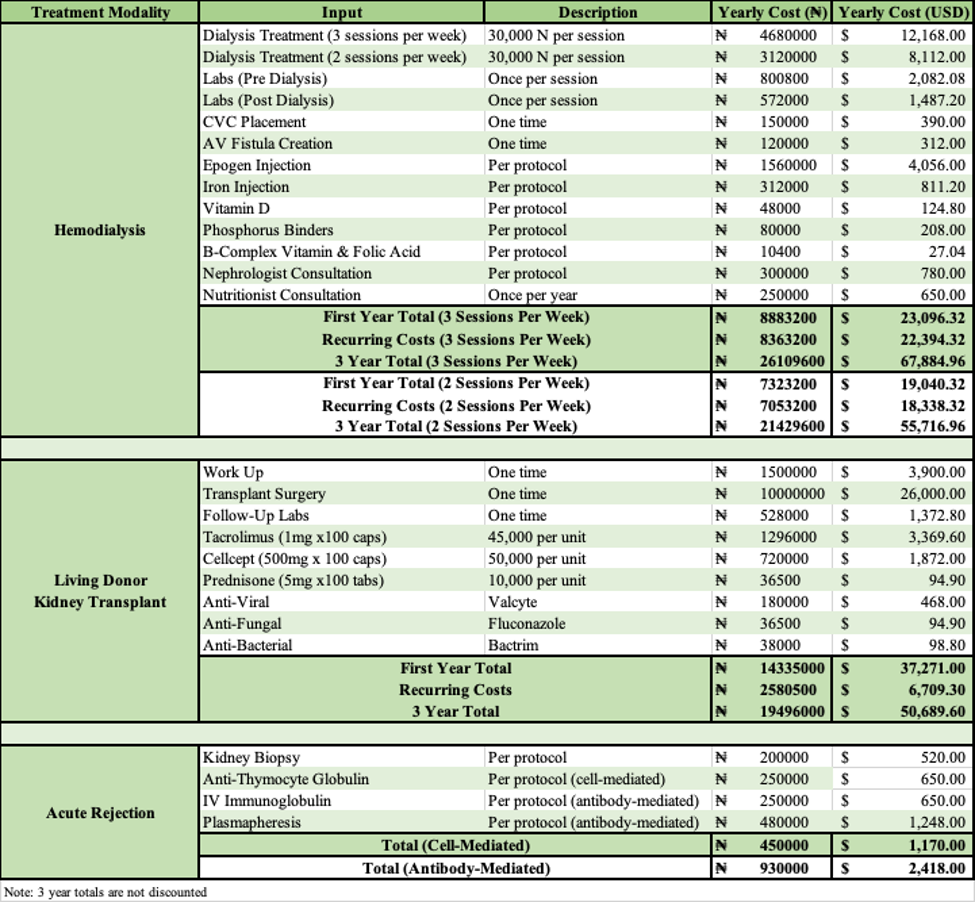
*Purpose: To primarily quantify the costs of LDKT and HD in Nigeria from a ‘payer’s perspective’ and secondarily inform future cost-effectiveness studies to guide health care decision-making of kidney disease management in the country.
*Methods: This study was conducted from a payer (the ESRD patient) perspective in Nigeria. Due to scarcity of aggregate costing data, direct costs were determined through expert consultation, supplier pricing, and patient utilization data. Data was obtained from 53 patients who underwent HD at centers across Nigeria from July 2014 to June 2020, and 20 patients with ESRD who received a LDKT between June 2017 and May 2020. Due to limited availability of services within Nigeria, costs are mostly fixed with little variation. A transplantation specialist, transplant nephrologist, and transplant coordinator were consulted to verify input variables and costs, as well as clinical pathways in ESRD. One year and yearly recurring costs of LDKT and HD were determined, with HD costs projected for both three sessions per week and two sessions per week. Cost of transplant rejection was also quantified but not included in one-year or recurring costs. Costs were converted to USD.
*Results: This cost comparison study demonstrated one-year costs of US $23,096.32 for HD (3 sessions per week) and $37,271.00 for LDKT. Yearly recurring costs were $22,394.32 for HD and $6,709.30 for LDKT. Costs of acute rejection for LDKT were $2,418.00 for antibody-mediated rejection and $1,170.00 for cell-mediated rejection. One-time costs dominated the one-year cost of LDKT at 82.0%, while alternatively 97.0% of one-year costs of HD were recurring costs. A discounted simulation (6% discount rate) of three-year costs when survival was assumed yielded a cost-savings of US $12,421.23 for LDKT in comparison to HD.
*Conclusions: Costs of LDKT in Nigeria are higher than that of HD in the first year but are markedly decreased in subsequent years. The cost of HD and LDKT is primarily an out-of-pocket expense paid by patients with kidney failure in Nigeria. The maintenance cost of HD is three times more than the maintenance cost of immunosuppression post kidney transplantation. Our data demonstrates favorable long-term cost profile of LDKT vs. HD in Nigeria when cost is borne directly by patients. Further study of the comparative cost-effectiveness of these RRT modalities using survival data and outcomes is necessary.
To cite this abstract in AMA style:
Lang J, James I, Afodu DDaRocha, Okwuonu CG, Ekwenna O. A Payer’s Perspective: The Cost of Hemodialysis versus Living Donor Kidney Transplant for Kidney Failure Patients in Nigeria [abstract]. Am J Transplant. 2021; 21 (suppl 3). https://atcmeetingabstracts.com/abstract/a-payers-perspective-the-cost-of-hemodialysis-versus-living-donor-kidney-transplant-for-kidney-failure-patients-in-nigeria/. Accessed May 31, 2026.« Back to 2021 American Transplant Congress