Maximizing Peri-Operative Value-Based Care in Kidney Transplant Induction
1Pharmacy, MUSC, Charleston, SC
2Surgery, MUSC, Charleston, SC
3Nephrology, MUSC, Charleston, SC.
Meeting: 2015 American Transplant Congress
Abstract number: A221
Keywords: Antilymphocyte antibodies, Kidney transplantation, Resource utilization, Simulect
Session Information
Session Name: Poster Session A: Non Organ Specific, Economics, Public Policy, Allocation, Ethics
Session Type: Poster Session
Date: Saturday, May 2, 2015
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Exhibit Hall E
Due to the dwindling reimbursement for kidney transplants (KTx), there must be a continuous effort to provide the best value-based care. The purpose of this study was to compare the cost-efficiency of two induction therapy protocols that have demonstrated equivalent efficacy.
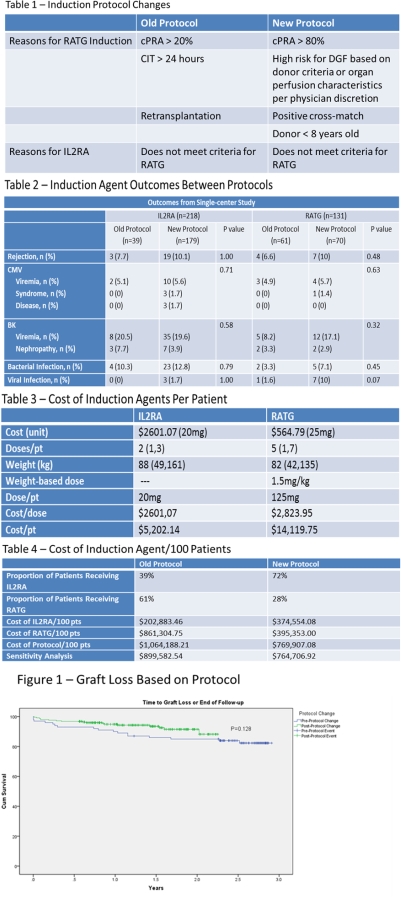
METHODS: A cost-minimization analysis was performed from the societal perspective comparing two distinct induction therapy protocols. The efficacy data was compiled from a single center retrospective cohort study of adult KTxs comparing two induction protocols between 8/2011-12/2013. A protocol revision in 2012 adjusted the targeted population for rabbit antithymocyte globulin (RATG) induction to high immunologic risk recipients (Table 1). Direct medication cost was taken from the wholesale acquisition cost (WAC) for the medications. We also performed a sensitivity analysis, in which cost savings was analyzed if the IL2RA were to cost 25% more and if the RATG were to cost 25% less. The results of this study were expressed in median cost per 100 patients treated according to each protocol.
RESULTS: Outcomes were equivalent between the two protocol groups (Table 2, Figure 1). Table 3 demonstrates the median WAC for each induction agent based on our patient population and protocol. RATG utilization decreased from 61% to 28%, while IL2RA increased from 39% to 72% (Table 3). The median WAC for induction agents per 100 pts decreased by 28% with the new protocol, saving approximately $294,281.13 to treat 100 patients. In our sensitivity analysis, the cost for induction agents per 100 pts in the new protocol remained 15% below the old protocol.
CONCLUSIONS: A data-driven protocol that reserves RATG for high-immunologic risk patients reduces medication costs by 28% while maintaining equivalent efficacy and safety. As the population of kidney transplant recipients is constantly changing, regular reanalysis and confirmation would be beneficial.
[figure2]
To cite this abstract in AMA style:
Fleming J, Casale J, Covert K, Boyle K, Taber D, Meadows H, Mardis C, Pilch N, Posadas-Salas M, Srinivas T, Bratton C, McGillicuddy J, Chavin K, Baliga P. Maximizing Peri-Operative Value-Based Care in Kidney Transplant Induction [abstract]. Am J Transplant. 2015; 15 (suppl 3). https://atcmeetingabstracts.com/abstract/maximizing-peri-operative-value-based-care-in-kidney-transplant-induction/. Accessed May 20, 2026.« Back to 2015 American Transplant Congress