Defining the Characteristics and Graft Outcomes of Kidney Transplant Recipients with Elevated Plasma Oxalate Level Not Due to Primary Hyperoxaluria
Mayo Clinic, Phoenix, AZ
Meeting: 2021 American Transplant Congress
Abstract number: 1054
Keywords: Kidney/liver transplantation, Nephropathy
Topic: Clinical Science » Kidney » Kidney Complications: Non-Immune Mediated Late Graft Failure
Session Information
Session Name: Kidney Complications: Non-Immune Mediated Late Graft Failure
Session Type: Poster Abstract
Session Date & Time: None. Available on demand.
Location: Virtual
*Purpose: Patients with elevated systemic oxalate burden due to enteric etiologies are at increased risk for calcium oxalate deposition causing ESRD. The objective of this study is to describe causes and graft function of kidney transplant (KTx) recipients with elevated plasma oxalate (Pox) not due to primary hyperoxaluria at our institution.
*Methods: KTx recipients between 2013 to 2019 with an elevated Pox at the time of KTx evaluation were included. Chart review was performed to evaluate for enteric causes. Patients with primary hyperoxaluria (PH) were excluded
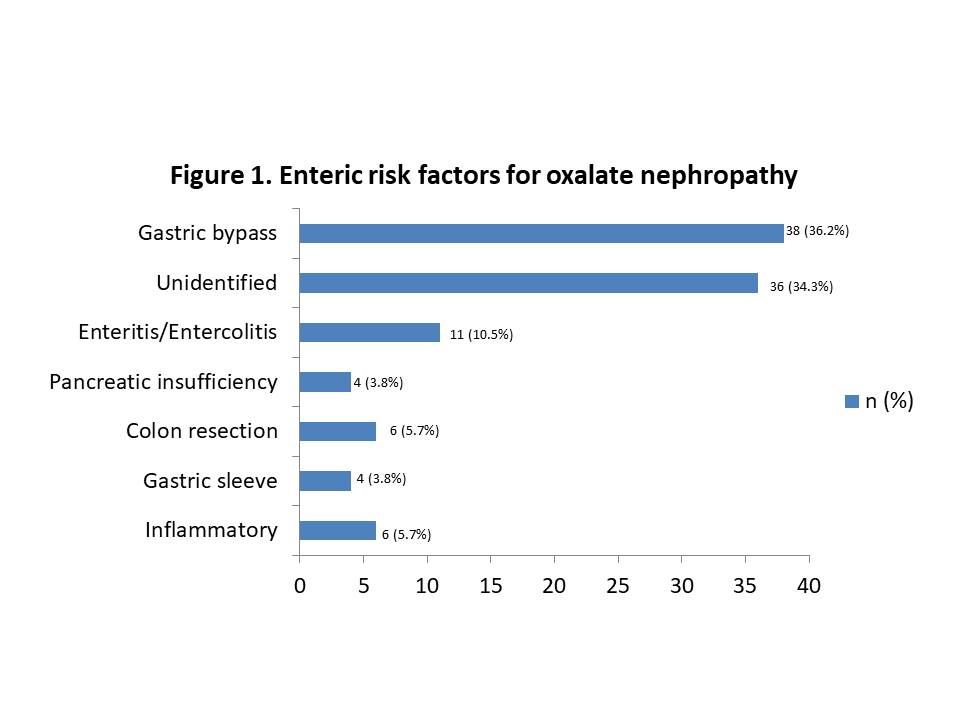
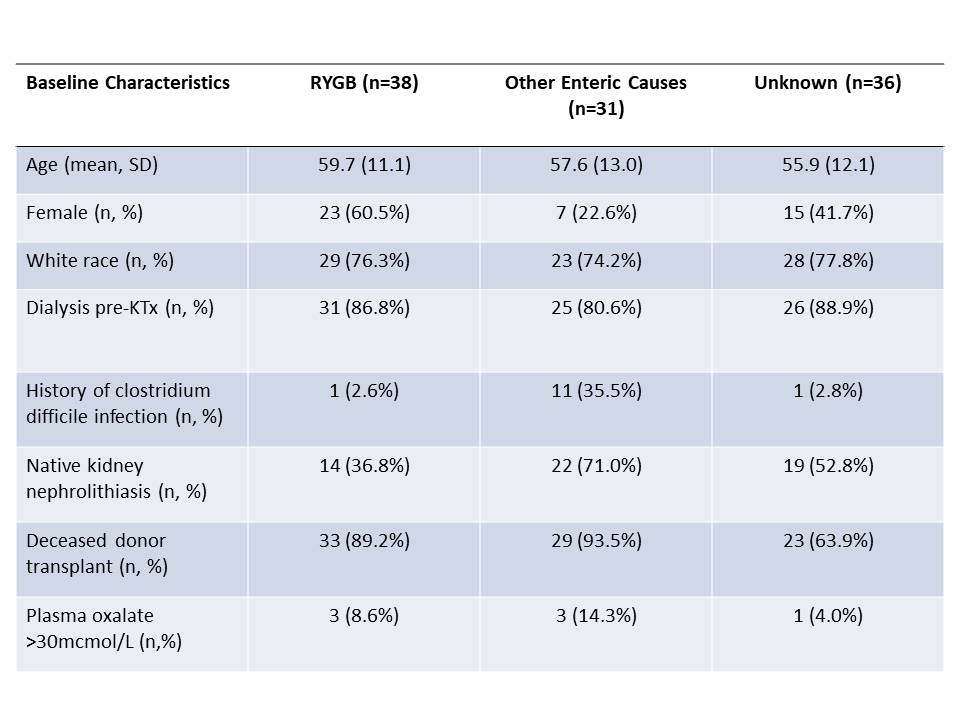
*Results: 105 patients were identified. Mean age was 57.8 years, 42.9% were female, 76.2% white, and 91.4% first KTx. The most common enteric cause was Roux-en-Y gastric bypass (RYGB, 36.2%) as shown in Figure 1. 34.3% did not have an identified cause. Baseline characteristics are shown in Table 1. Patients with RYGB were significantly more likely to have diabetes (65.8%, p=0.033) but less likely to have a history of nephrolithiasis(36.8%, p=0.019) compared to patients with either unidentified (diabetes:36.1%, nephrolithiasis:52.8%) or alternative enteric cause (diabetes:45.2%, nephrolithiasis:71%) of oxalosis. Patients with RYGB had significantly higher median Pox pre-KTX than either unidentified or alternative enteric cause (15.2mcmol/L compared to 6.1mcmol/L and 11.8mcmol/L, respectively) (p= 0.032). There was no significant difference in long-term transplant outcomes noted for patients regardless of the etiology of elevated POx (with the primary transplant outcome endpoint of GFR at 1yr post-KTx). One-year GFR for patients with RGYB was 50.2±21.9mL/min/1.73m2, compared to 53.2±18.0mL/min/1.73m2 and 48.8±23.4mL/min/1.73m2 for unknown and alternative enteric causes, respectively. Mean 1-year GFR for deceased donor KTx for our Transplant Center is 58.9 ±20.6ml/min/1.73m2.
*Conclusions: RYGB is the most common cause of enteric oxalosis in KTx recipients but in a third of cases, an enteric cause was never identified. There was no significant difference in GFR between the three groups; however, all groups had a lower GFR compared to the mean GFR of our transplant Center. Further studies are needed to assess the risk of enteric risk factors on long-term graft function.
To cite this abstract in AMA style:
Khan D, Zhang N, Keddis M. Defining the Characteristics and Graft Outcomes of Kidney Transplant Recipients with Elevated Plasma Oxalate Level Not Due to Primary Hyperoxaluria [abstract]. Am J Transplant. 2021; 21 (suppl 3). https://atcmeetingabstracts.com/abstract/defining-the-characteristics-and-graft-outcomes-of-kidney-transplant-recipients-with-elevated-plasma-oxalate-level-not-due-to-primary-hyperoxaluria/. Accessed May 25, 2026.« Back to 2021 American Transplant Congress