Effect of Induction Therapy on Absolute CD4 Count and CD4 Percentage in HIV Positive Kidney Transplant Recipients
1Pharmacy, Houston Methodist Hospital, Houston, TX, 2Surgery, Houston Methodist Hospital, Houston, TX
Meeting: 2019 American Transplant Congress
Abstract number: B227
Keywords: CD4, HIV virus, Induction therapy
Session Information
Session Name: Poster Session B: Kidney Infections
Session Type: Poster Session
Date: Sunday, June 2, 2019
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:00pm-7:00pm
Presentation Time: 6:00pm-7:00pm
Location: Hall C & D
*Purpose: Anti-thymocyte globulin (ATG) induction causes profound and long-lasting lymphocyte depletion, with CD4+ reconstitution lagging behind other subsets. While absolute CD4 count is the preferred monitoring parameter for disease progression and immune function in HIV (+) patients, lymphocyte-depleting induction may render it unreliable as a marker in HIV (+) transplant recipients. CD4 percentage (%CD4) of lymphocytes could be a reasonable alternative. Herein we describe the pattern of absolute CD4 count and %CD4 recovery following ATG induction.
*Methods: We performed a single-center review of HIV (+) kidney transplant recipients from 2007 to 2017. Patients with lymphocyte subset data available at our institution were included. Recovery at 1 year post-transplant was defined according to AIDS definitions established by the CDC, as an absolute CD4 count ≥200 cells/µL and CD4 percentage ≥14%.
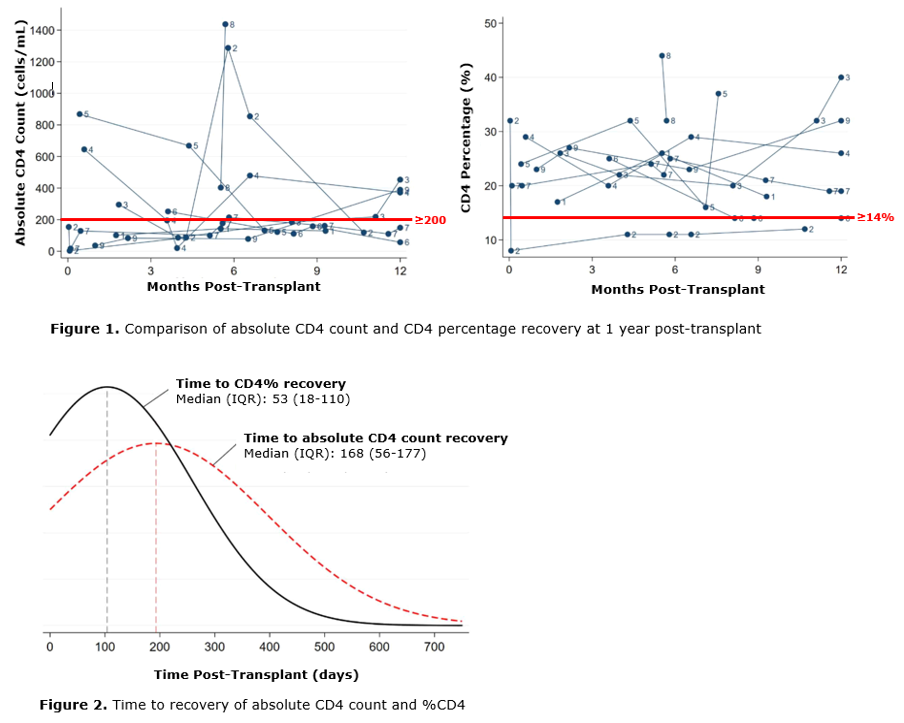
*Results: A total of 25 HIV(+) patients were identified, of which 9 with CD4 monitoring were included. Mean age was 48±8 years, 6 male, 5 African American, and 6 deceased donor kidney transplants. All patients received ATG induction followed by maintenance immunosuppression with tacrolimus, mycophenolate mofetil, and prednisone. At 1 year, 8 (89%) had an absolute CD4 count ≥200 and 8 (89%) had %CD4 ≥14%. Individual patient trends are depicted in Figure 1. Absolute CD4 count and %CD4 recovery were discordant in 2 cases; 1 patient had recovery of CD4 count but not %CD4, whereas the other had %CD4 recovery but not absolute CD4 count. Median times to recovery of absolute CD4 count and %CD4 were 168 (IQR 56-177) and 53 (IQR 18-110) days, respectively (Figure 2). No breakthrough HIV viremia occurred; there was one case of HSV esophagitis but no other opportunistic infections. There were no graft losses or patient deaths at 1 year.
*Conclusions: These data suggest that although adequate recovery of both absolute CD4 count and %CD4 were observed following ATG induction, discordance between the values may exist. Furthermore, %CD4 may recover earlier than absolute counts. To our knowledge, this is the first study to assess the role of monitoring %CD4 in HIV (+) transplant recipients. Understanding lymphocyte reconstitution and the utility of %CD4 monitoring requires further investigation.
To cite this abstract in AMA style:
Kuten SA, Dunne IE, Cantwell AE, Hobeika MJ, Yi SG, Musick W, Knight RJ, Gaber AO. Effect of Induction Therapy on Absolute CD4 Count and CD4 Percentage in HIV Positive Kidney Transplant Recipients [abstract]. Am J Transplant. 2019; 19 (suppl 3). https://atcmeetingabstracts.com/abstract/effect-of-induction-therapy-on-absolute-cd4-count-and-cd4-percentage-in-hiv-positive-kidney-transplant-recipients/. Accessed May 16, 2026.« Back to 2019 American Transplant Congress