The Impact of Early versus Late Clinical Outcomes on Disparities in African-American Kidney Transplant Recipients
MUSC, Charleston, SC.
Meeting: 2018 American Transplant Congress
Abstract number: 158
Keywords: African-American, Graft survival, Kidney transplantation
Session Information
Session Name: Concurrent Session: Non-Organ Specific: Disparities to Outcome and Access to Healthcare
Session Type: Concurrent Session
Date: Sunday, June 3, 2018
Session Time: 4:30pm-6:00pm
 Presentation Time: 5:42pm-5:54pm
Presentation Time: 5:42pm-5:54pm
Location: Room 4C-4
Background: It is important to better understand the impact of early and late clinical events on disparities in African-American (AA) kidney transplant (KTX), which will allow for the development and testing of focused interventions aimed at mitigating differences by race.
Methods: Longitudinal cohort study of adult KTX transplanted between 2007-16 followed through Aug 2017. Detailed clinical data, including rejection events (rej), systolic blood pressures (SBPs), glucoses, hemoglobins (Hgbs) and tacrolimus (FK) levels were electronically abstracted from the EHR. Clinical data and events were classified as early (within 2 yrs of transplant) or late (after 2 yrs post-transplant). Clinical events were defined as acute rej (Banff ≥1A), mean SBP >140 mmHg, high FK variability (CV) >40%, mean glucose >160 mg/dL and mean Hgb <10 gm/dL. Iterative multivariable competing risk Cox regression modelling was utilized to assess the impact of early vs. late events on racial disparities in AA KTX.
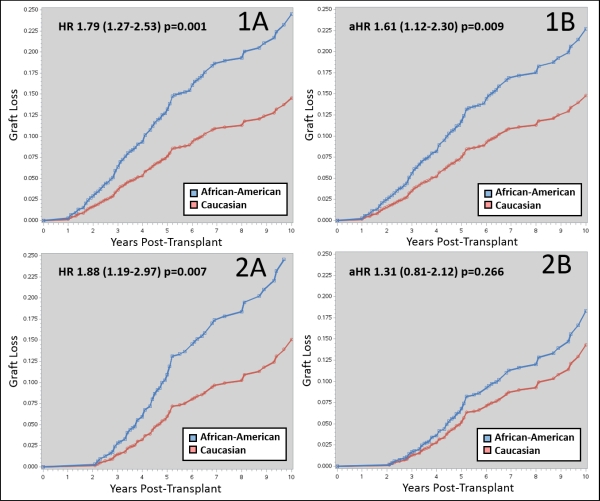
Results: 1,610 KTX were assessed (54.2% AAs), with 1,359 in the early events complete case cohort and 793 in the late events complete case cohort. AAs had 49% higher risk of early clinical events (RR 1.49, 1.28-1.76; p<0.001), and 69% higher risk of late clinical events (RR 1.69, 1.33-2.15; p<0.001). Early lack of rej and control of SBP, glucoses, FK variability and Hgb reduced the absolute risk of graft loss in AAs by 18% (HR from 1.79 to 1.61, Figures 1A and 1B), while lack of late rej and control of late SBPs, glucoses, FK variability and Hgbs reduced the absolute risk of graft loss in AAs by 57% (HR from 1.88 to 1.31, Figures 2A and 2B). Iterative nested models demonstrated that prevention of late rejection and obtaining late SBP control were the clinical events that had the largest impact on racial disparities.
Conclusion: Based on these results, it appears that focusing efforts to reduce late acute rejections and improve control of late SBPs, glucoses, FK variability and anemia will have more impact on reducing racial disparities in AA KTX, as compared to focusing on early events.
CITATION INFORMATION: Taber D., Fleming J., Su Z., Mauldin P., McGillicuddy J., Nadig S., Rohan V., Baliga P., Dubay D. The Impact of Early versus Late Clinical Outcomes on Disparities in African-American Kidney Transplant Recipients Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Taber D, Fleming J, Su Z, Mauldin P, McGillicuddy J, Nadig S, Rohan V, Baliga P, Dubay D. The Impact of Early versus Late Clinical Outcomes on Disparities in African-American Kidney Transplant Recipients [abstract]. https://atcmeetingabstracts.com/abstract/the-impact-of-early-versus-late-clinical-outcomes-on-disparities-in-african-american-kidney-transplant-recipients/. Accessed May 24, 2026.« Back to 2018 American Transplant Congress