Pre-Transplant Loco-Regional Therapy for Hepatocellular Carcinoma and Post-Transplant Outcomes: A National Study.
1Saint Louis Univ, Saint Louis
2East Carolina Univ, Greenville.
Meeting: 2016 American Transplant Congress
Abstract number: 105
Keywords: Hepatocellular carcinoma, Liver transplantation, Outcome, Survival
Session Information
Session Name: Concurrent Session: Hepatic Malignancies
Session Type: Concurrent Session
Date: Sunday, June 12, 2016
Session Time: 4:30pm-6:00pm
 Presentation Time: 4:42pm-4:54pm
Presentation Time: 4:42pm-4:54pm
Location: Room 304
Currently most transplant centers use loco-regional therapy to bridge liver transplant (LT) candidates with hepatocellular carcinoma (HCC). However, limited data are available to support the efficacy of these approaches.
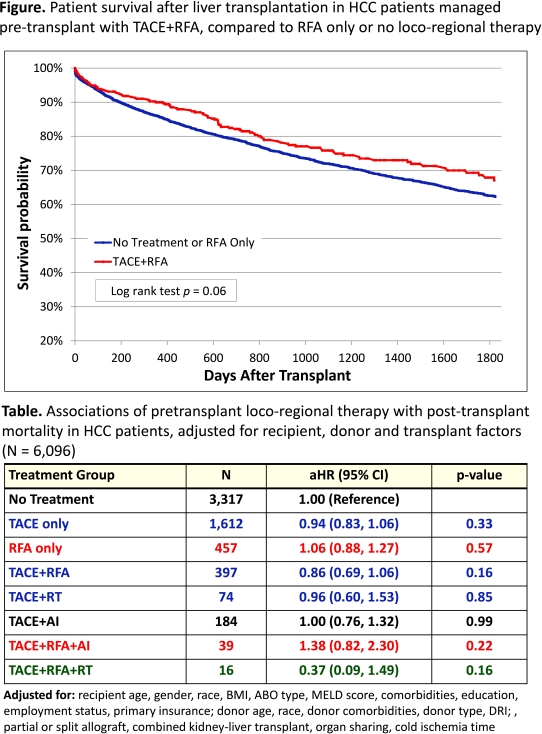
We examined a novel linkage of the Organ Procurement Transplant Network (OPTN) registry and Medicare claims data for 18,945 LT recipients (2003-2013) with HCC as the primary diagnosis for LT (N=6,096). Loco-regional therapy in the year before LT was identified based on International Classification of Diseases (ICD)-9 procedure and Common Procedural Terminology (CPT) codes in the year before transplantation, and categorized as: trans-arterial chemoembolization (TACE), radio-frequency ablation (RFA) only, or combination therapies including radiotherapy (RT), RFA or alcohol injection (AI). Associations of loco-regional regimen with 5-yr post-LT mortality was examined by multivariate Cox regression. A secondary analysis was performed among those with explant pathology adjusting for tumor size, number, presence of vascular invasion, and differentiation as reported to the OPTN (N=1,674).
LT recipients with HCC managed with TACE+RFA pre-transplant had qualitatively superior post-LT survival compared to patients managed with RFA alone or no loco-regional therapy (Kaplan-Meier P=0.06) (Figure). After adjustment for baseline recipient, donor and transplant factors, compared with no loco-regional therapy, most single or combination therapies were associated with trends lower post-transplant mortality except TACE+AI (Table). However, the favorable patterns did not reach statistical significance. Patterns were similar in the subgroup with explant pathology records.
Combination loco-regional prior to transplant might improve post-transplant survival among LT candidates with HCC. In light of new US allocation policy for HCC exception scores expected to lengthen waiting time for many HCC patients, ongoing studies are vital to define the optimal management of patients with HCC before and after LT.
CITATION INFORMATION: Nazzal M, Chen J, Lentine K, Schnitzler M, Tuttle-Newhall J, Varma C, Taha A, Said A, Xiao H, Randall H. Pre-Transplant Loco-Regional Therapy for Hepatocellular Carcinoma and Post-Transplant Outcomes: A National Study. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Nazzal M, Chen J, Lentine K, Schnitzler M, Tuttle-Newhall J, Varma C, Taha A, Said A, Xiao H, Randall H. Pre-Transplant Loco-Regional Therapy for Hepatocellular Carcinoma and Post-Transplant Outcomes: A National Study. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/pre-transplant-loco-regional-therapy-for-hepatocellular-carcinoma-and-post-transplant-outcomes-a-national-study/. Accessed May 19, 2026.« Back to 2016 American Transplant Congress