Comparative Effectiveness of Cytomegalovirus Prevention Strategies in a Large Retrospective Cohort of Kidney Transplant Recipients.
Washington University School of Medicine, Saint Louis, MO.
Meeting: 2016 American Transplant Congress
Abstract number: C284
Keywords: Cytomeglovirus, Prophylaxis
Session Information
Session Name: Poster Session C: Viruses and SOT
Session Type: Poster Session
Date: Monday, June 13, 2016
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:00pm-7:00pm
Presentation Time: 6:00pm-7:00pm
Location: Halls C&D
Background: While CMV prevention strategies have been studied in carefully selected groups of patients enrolled in randomized trials, their comparative effectiveness in real-world settings is unknown.
Methods: We assembled a cohort of 16,713 kidney transplant recipients with Medicare Part D coverage from 2006-2011 using USRDS data, and compared the incidence of active CMV infection, allograft failure or death among propensity score matched cohorts of D+/R-, R+ and D-/R- patients who either used or did not use CMV prophylaxis. CMV prophylaxis was defined as filled prescriptions for prophylactic-dose valganciclovir, ganciclovir or valacyclovir within 28 days of transplant; active CMV infection was defined as inpatient ICD-9-CM coding for CMV, or outpatient use of treatment-dose valganciclovir, ganciclovir, foscarnet or cidofovir; and allograft failure or death was defined as dialysis, UNOS-reported transplant failure, repeat kidney transplant or death. Non-parsimonious logistic regression models predicted the propensity for CMV prophylaxis, and outcomes were compared using Kaplan-Meier curves and log-rank testing.
Results: CMV prophylaxis was prescribed to 72% of D+/R- patients, 63% of R+ patients and 36% of D-/R- patients. Active CMV infection was identified in 23% of D+/R- patients, 8% of R+ patients and 5% of D-/R- patients. Allograft failure or death was identified in 13% of D+/R- patients, 12% of R+ patients and 11% of D-/R- patients. CMV prophylaxis was associated with less active CMV infection, and allograft failure or death in R+ patients, but not D+/R- or D-/R- patients. 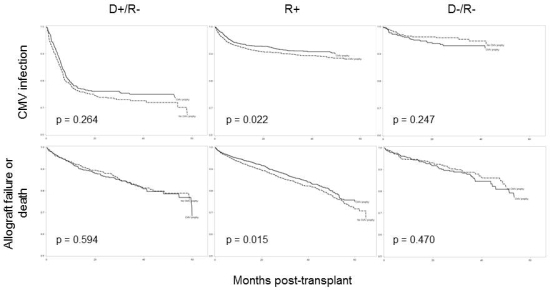
Conclusions: CMV prophylaxis is protective against active CMV infection, allograft failure or death in R+ patients, but not D+/R- or D-/R- patients in real-world settings. Better CMV prevention strategies should be developed for D+/R- patients given their continued high risk of CMV disease that occurs after prophylaxis is discontinued. CMV prophylaxis is unnecessary in D-/R- patients given their minimal risk of developing CMV disease.
CITATION INFORMATION: Santos C, Saeed M, Brennan D, Olsen M. Comparative Effectiveness of Cytomegalovirus Prevention Strategies in a Large Retrospective Cohort of Kidney Transplant Recipients. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Santos C, Saeed M, Brennan D, Olsen M. Comparative Effectiveness of Cytomegalovirus Prevention Strategies in a Large Retrospective Cohort of Kidney Transplant Recipients. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/comparative-effectiveness-of-cytomegalovirus-prevention-strategies-in-a-large-retrospective-cohort-of-kidney-transplant-recipients/. Accessed May 11, 2026.« Back to 2016 American Transplant Congress