Same Policy, Different Impact: Center and Regional Effects of SHARE 35 Liver Allocation.
1Surgery, University of Pennsylvania, Philadelphia, PA
2Medicine, University of Pennsylvania, Philadelphia, PA.
Meeting: 2016 American Transplant Congress
Abstract number: B241
Keywords: Allocation, Liver transplantation
Session Information
Session Name: Poster Session B: Liver: MELD, Allocation and Donor Issues (DCD/ECD)
Session Type: Poster Session
Date: Sunday, June 12, 2016
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:00pm-7:00pm
Presentation Time: 6:00pm-7:00pm
Location: Halls C&D
Introduction: Early studies of national data suggest that Share-35 implementation was associated with more liver transplants, fewer discards, and lower waitlist mortality, without worsening of post-transplant outcomes. Patterns of utilization of Share-35 at a regional and center specific level remain unknown.
Methods: United Network for Organ Sharing data was analyzed to compare liver transplant recipients with allocation-MELD (aMELD) ≥35 from the two years prior and the one year after Share-35 implementation.
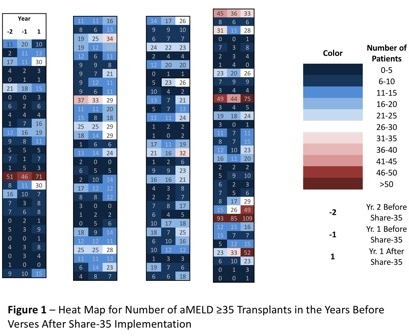
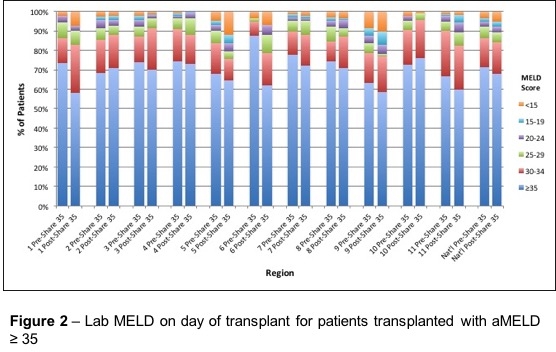
Results: Analysis revealed among-center variation in the number and proportion of aMELD ≥35 transplants pre- versus post-Share-35. While most centers saw minimal volume changes, there were nine centers with a ≥15 increase in aMELD ≥35 transplants the year after implementation (Figure 1). The top 10 centers, determined by the largest increase in aMELD ≥35 transplants from the year before to the year after Share-35, accounted for 66.1% of the total national increase in aMELD ≥35 transplants. Day of transplant true lab MELD scores for patients transplanted with aMELD ≥ 35 were compared pre- versus post-Share-35. In most regions, the percent of patients who had a true lab MELD ≥35 on their day of transplant decreased (Figure 2), and nationally, the percentage of patients decreased from 67.8% pre- to 66.4% post-Share 35.
Conclusion: There was significant variation in the volume changes of aMELD ≥35 transplants between centers, with the majority of the increase in volume attributable to a few centers. Longer term data is needed to assess whether the outcome for patients in centers with large volume increases are equivalent to other aMELD ≥35 patients, and what factors in listing, organ access, or center aggressiveness are contributing to these differences.
CITATION INFORMATION: Murken D, Peng A, Aufhauser Jr D, Goldberg D, Levine M. Same Policy, Different Impact: Center and Regional Effects of SHARE 35 Liver Allocation. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Murken D, Peng A, Jr DAufhauser, Goldberg D, Levine M. Same Policy, Different Impact: Center and Regional Effects of SHARE 35 Liver Allocation. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/same-policy-different-impact-center-and-regional-effects-of-share-35-liver-allocation/. Accessed April 30, 2026.« Back to 2016 American Transplant Congress