Impact of Donor Specific Antibodies on Cardiac Allograft Vasculopathy.
1University of Pittsburgh Medical Center, Pittsburgh, PA
2Heart and Vascular Institute, University of Pittsburgh Medical Center, Pittsburgh, PA
3Pathology Department, University of Pittsburgh, Pittsburgh, PA.
Meeting: 2016 American Transplant Congress
Abstract number: B156
Keywords: Alloantibodies, Arteriosclerosis, Heart transplant patients, HLA antibodies
Session Information
Session Name: Poster Session B: Hearts and VADs in Depth - The Force Awakens
Session Type: Poster Session
Date: Sunday, June 12, 2016
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:00pm-7:00pm
Presentation Time: 6:00pm-7:00pm
Location: Halls C&D
Purpose: Cardiac allograft vasculopathy (CAV) is a significant complication after cardiac transplantation (CTX). The presence of donor specific antibodies (DSA) has been associated with an increased incidence of CAV in cardiac transplant (CTX) patients.
Methods: A retrospective analysis of prospectively collected data for all CTX recipients at a single center from 2008-2015 who had at least one angiogram and donor specific HLA-antibody (DSA) measured. Luminex single antigen bead assays were used to assess DSAs per protocol up to 6 months then yearly after transplant. CAV is defined as a ≥30% stenosis of any primary vessel.
Results: This study included 262 CTX recipients, 45 (17.2%) developed any DSA, 19 (7.25%) developed Class I DSA, and 38 (14.5%) developed Class II DSA. Patients were median age of 57.3 years, 79.4% male, and 91.2% Caucasian. Those who developed Class I DSA were younger (median age 52.3 v. 57.6 years, p=0.011) and have higher Class I PRA at transplant (10.0 versus 2.0, p=0.003). There was no difference in characteristics for those who did and did not develop Class II PRA. 14/45 patients (31%) with any DSA developed CAV compared to 31/217 (14.3%) without DSA. 6/19 patients (31.5%) with Class I DSA developed CAV while 39/243 (16.0%) of patients without Class I DSA developed CAV. The presence of any DSA was associated with CAV. Specifically Class I DSA was associated with a 4.69 times increased risk of developing CAV (p=0.011). The presence of any Class II DSA did not significantly increase the risk of developing CAV (HR= 1.93, p=0.38).
Time to development of CAV is represented in Figure 1. The 6 year incidence of CAV in patients with any DSA, Class I DSA, and Class II DSA are 41%, 50%, and 41% respectively. 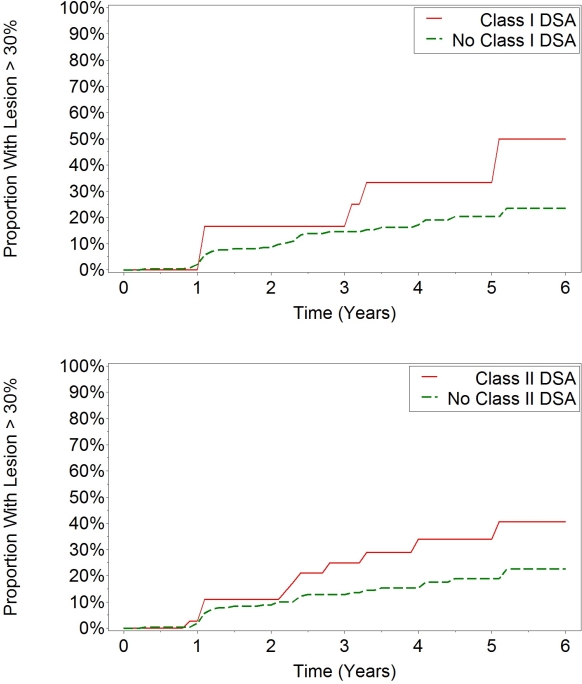
Conclusion: Patients with Class I DSA are at a higher risk of developing CAV compared to patients without DSA.
CITATION INFORMATION: Vu A, Althouse A, Zeevi A, Teuteberg J, Shullo M. Impact of Donor Specific Antibodies on Cardiac Allograft Vasculopathy. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Vu A, Althouse A, Zeevi A, Teuteberg J, Shullo M. Impact of Donor Specific Antibodies on Cardiac Allograft Vasculopathy. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/impact-of-donor-specific-antibodies-on-cardiac-allograft-vasculopathy/. Accessed April 22, 2026.« Back to 2016 American Transplant Congress