Transplant Center Volume in High-risk Donors are Associated with Graft and Patient Survival
Transplant, Washington University, Saint Louis, MO
Meeting: 2021 American Transplant Congress
Abstract number: 851
Keywords: Donors, non-heart-beating, Kidney transplantation, Survival
Topic: Clinical Science » Kidney » Kidney Deceased Donor Selection
Session Information
Session Name: Kidney Deceased Donor Selection
Session Type: Poster Abstract
Session Date & Time: None. Available on demand.
Location: Virtual
*Purpose: Evaluation of high-risk kidney donors in transplant centers involves an intensive assessment of the individual risks and selection of appropriate recipients. Understandably, this requires well thought out protocols and structures to maintain good outcomes. In this study, we explore the association of center volume with patient and graft survival in high risk donor transplants.
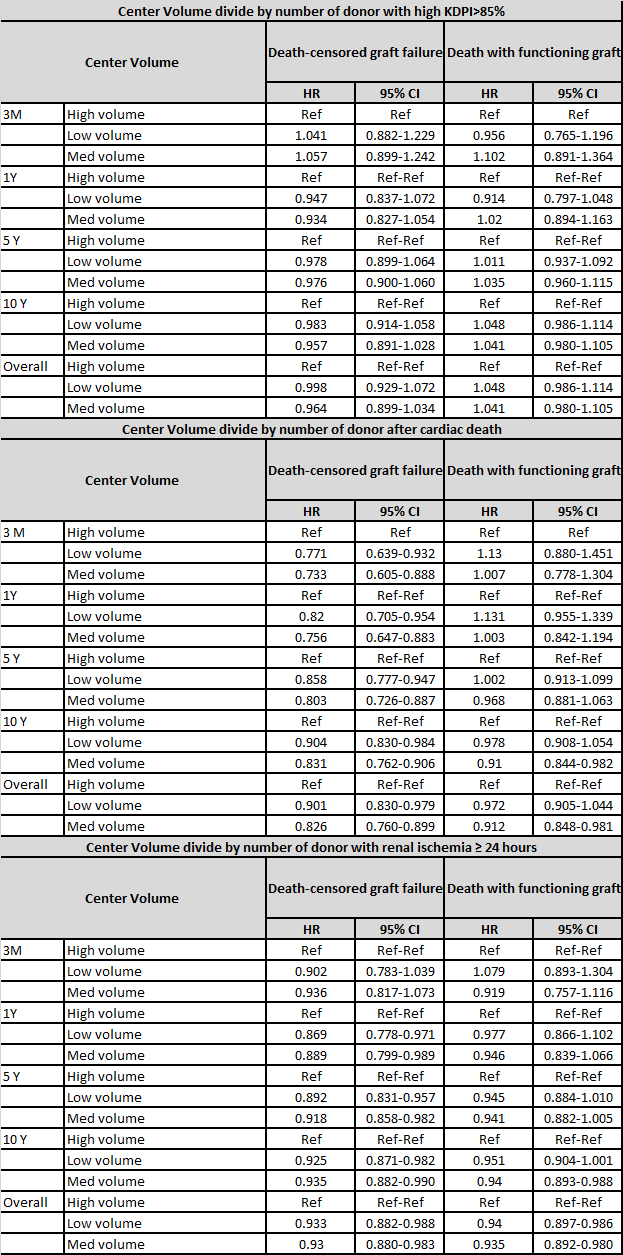
*Methods: We reviewed Organ Procurement and Transplantation Network (OPTN) data on kidney transplants among 285 transplant centers between 2000 and 2016. High-risk kidney transplant included donation after cardiac death (DCD), cold ischemic time≥24 hours and high KDPI≥85%. For each high-risk transplant, transplant centers were categorized into tertiles of low, medium and high volume according to the annual average transplant volume of such transplant. The outcomes were death censored graft loss (DCGL) and death with functioning graft (DWFG). The association of center volume with each outcome was analyzed using multivariable Cox regression including adjustment for recipient, donor, and transplant characteristics.
*Results: Compared to high volume centers, the lower and medium center volume for DCD kidneys had a lower risk for DCGL at 3 months (aHR=0.771[0.639-0.932]; aHR=0.733[0.605-0.888]) longer follow up at 1, 5 and 10 years and overall have similar trends. There was only lower risk for DWFG for medium center volume DCD in 10 years aHR=0.910(0.844-0.982) and overall aHR=0.912 (0.848-0.981). For lower volume and medium volume with cold ischemic time ≥ 24 hours there was lower risk for DCGL at 1 year (aHR=0.869[0.778-0.971];aHR=0.889[0.799-0.989]), 5 years (aHR=0.892[0.831-0.957];aHR=0.918[0.858-0.982]); 10 years (aHR=0.925[0.871-0.982];aHR=0.935[0.882-0.990]) and overall (aHR=0.933[0.882];aHR=0.930[0.880-0.983]) when compare high center volume. In low and medium center volumes for prolonged cold ischemic time there was a lower risk for DWFG overall (aHR= 0.940[0.897-0.986]; aHR=0.933[0.892-0.980]) when compared with high center volume. We observed that lower and medium center volume in kidney with a KDPI≥85% were not associated with higher risk for DCGL and DWFG.
*Conclusions: We found that DCD and cold ischemic time≥24 hour had a worse DCGL in high volume centers but not in kidney with high KDPI≥ 85%. Large studies with prospective follow up are needed to determine donor characteristics of DCD and cold ischemic time>24 hours that lead to greater risk for DCGL in high volume centers.
To cite this abstract in AMA style:
Merzkani MA, Murad H, Mattu M, Wang M, Hu V, Chang S, Alhamad T. Transplant Center Volume in High-risk Donors are Associated with Graft and Patient Survival [abstract]. Am J Transplant. 2021; 21 (suppl 3). https://atcmeetingabstracts.com/abstract/transplant-center-volume-in-high-risk-donors-are-associated-with-graft-and-patient-survival/. Accessed March 24, 2026.« Back to 2021 American Transplant Congress