The US Kidney Allocation System Should Not Allocate En Bloc Kidneys from Deceased Donors < 18 Kg as Equivalent to Top 20% KDPI Single Kidneys
1University of Chicago, Chicago, IL, 2Stanford University, Palo Alto, CA
Meeting: 2022 American Transplant Congress
Abstract number: 707
Keywords: Allocation, Kidney, Pediatric, Procurement
Topic: Clinical Science » Kidney » 31 - Kidney Deceased Donor Allocation
Session Information
Session Name: Kidney Deceased Donor Allocation
Session Type: Poster Abstract
Date: Saturday, June 4, 2022
Session Time: 5:30pm-7:00pm
 Presentation Time: 5:30pm-7:00pm
Presentation Time: 5:30pm-7:00pm
Location: Hynes Halls C & D
Session Information
Session Time: 7:00pm-8:00pm
Presentation Time: 7:00pm-8:00pm
Location: Hynes Hall C
*Purpose: In December 2020, the US Kidney Allocation System (KAS) revised the allocation rules for deceased donors under 18 kg, stating that both kidneys must be offered en bloc in the same allocation sequence as kidneys from donors with a Kidney Donor Profile Index (KDPI) < 20%. However, it is unknown if these small en bloc grafts are functionally equivalent to the highest-quality single kidney grafts.
*Methods: We extracted data on all deceased donor kidney-alone transplants from 12/4/2010 to 12/4/2019 from the Scientific Registry of Transplant Recipients. The primary outcome was time to graft failure or death with a functioning graft. We estimated the graft survival functions of en bloc grafts from donors < 18 kg and SKTs by KDPI sequence with the Kaplan-Meier method and compared graft survival at 1, 3, and 5 years. For each graft type, we calculated the 5-year restricted mean survival time (equivalent to the area under the Kaplan-Meier curve) and estimated differences in the average number of days of graft survival in the first 5 years, adjusting for recipient age, dialysis time, diabetic status, and history of previous organ transplant characteristics and time period (before or after the 2014 KAS update).
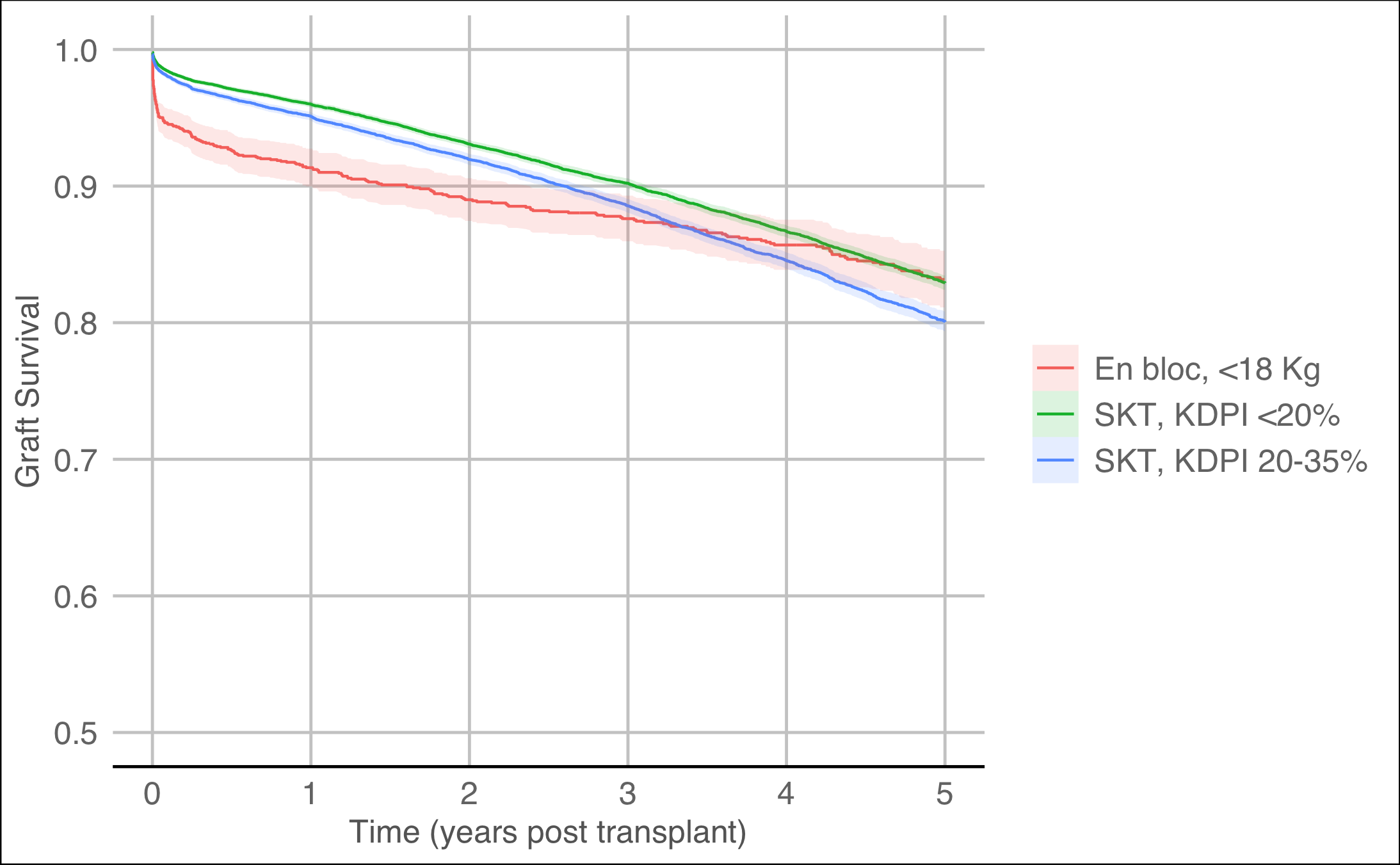
*Results: In the study time period, there were 115,143 deceased donor kidney transplants, 1,604 using kidneys procured en bloc from donors under 18 Kg. The Figure shows graft survival of en bloc kidney transplants from donors under 18 kg compared to Single Kidney Transplants (SKT) in sequence A (KDP < 20%) and sequence B (KDPI 20-35%). At 90-days post-transplantation, 6% of en bloc grafts from donors under 18 Kg had failed compared to only 2% of SKT from donors with KDPI <20% (p <0.01). At three years, graft survival of en bloc grafts from donors under 18 Kg was 88% compared to 90% for SKT from donors with KDPI < 20% (p <0.01). Adjusted for recipient covariates and time period, en bloc grafts from deceased donors under 18 kg had 51.4 fewer days of graft survival in the first 5 years post-transplantation compared to SKT with KDPI < 20% (p < 0.01).
*Conclusions: Deceased donor kidney grafts procured en bloc from donors < 18 kg have a higher risk of immediate graft failure and significantly worse aggregate performance across the first five years following transplantation compared to SKT from donors with KDPI < 20%. The policy of allocating en bloc grafts from donors <18 kg as equivalent to top-quality single kidneys may undermine the OPTN policy of offering the “best” kidneys to the candidates with the highest expected post-transplant survival.
To cite this abstract in AMA style:
Parker WF, Gallo A, Ross L. The US Kidney Allocation System Should Not Allocate En Bloc Kidneys from Deceased Donors < 18 Kg as Equivalent to Top 20% KDPI Single Kidneys [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/the-us-kidney-allocation-system-should-not-allocate-en-bloc-kidneys-from-deceased-donors-18-kg-as-equivalent-to-top-20-kdpi-single-kidneys/. Accessed April 10, 2026.« Back to 2022 American Transplant Congress