Risk of Amiodarone and Permanent Pacemaker Placement After Heart Transplantation.
Cedars-Sinai Heart Institute, Los Angeles
Meeting: 2017 American Transplant Congress
Abstract number: C108
Keywords: Heart transplant patients
Session Information
Session Name: Poster Session C: Hearts and VADS: All Topics
Session Type: Poster Session
Date: Monday, May 1, 2017
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:00pm-7:00pm
Presentation Time: 6:00pm-7:00pm
Location: Hall D1
Background: Patients (pts) with end stage heart disease undergoing heart transplantation (HT) may be on amiodarone (AD) for arrhythmias. AD may persist for weeks after HT due to a long half-life and large volume of distribution. AD may affect donor heart rate (HR) and cause bradycardia. Therefore, we assessed HT pts previously on AD for early post-HT negative chronotropic effects.
Methods: Between 2010-15 we identified 73 pts who were on various doses of AD just prior to HT with at least 6-month duration of medication use. HR was monitored within 60 days post-HT recording the slowest HR, need for permanent pacemaker (PPM), and need for terbutaline therapy. These pts were compared to those who did not use AD prior to HT. Endpoints included 60 day freedom from need for terbutaline, 1-yr freedom from PPM, 1-yr freedom from severe primary graft dysfunction, 1-yr survival, 1-yr freedom from cardiac allograft vasculopathy as defined by stenosis ≥30% by angiography and 1-yr freedom from Non-Fatal Major Adverse Cardiac Events (NF-MACE: myocardial infarction, new congestive heart failure, percutaneous coronary intervention, implantable cardioverter defibrillator implant, stroke) and treated rejection (TR).
Results: AD pts compared to non-AD pts had significantly lower freedom from PPM (90.9% vs 97.5%, p=0.015). AD pts had a mean minimum HR of 77bpm±10 (transient). The use of terbutaline in the AD pts was 60.3% (44/73) with a mean minimum HR of 69bpm±8 prior to use, rising to a mean HR of 79bpm±10 after terbutaline (p<0.001). There was significantly reduced 1-yr freedom from CAV in the AD group compared to the control (83.5% vs 95.3%, p<0.001) but there were more CMV mismatched pts in the AD group (37.5% vs 18.8%, p=0.001). There was no difference in 1-yr survival, freedom from NFMACE or TR.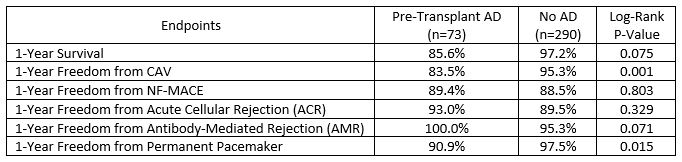 Conclusion: AD use prior to HT is associated with increased need for PPM after HT despite use of terbutaline which does appear to have a significant effect to increase HR. The increased risk for first yr CAV development in AD pts requires further investigation.
Conclusion: AD use prior to HT is associated with increased need for PPM after HT despite use of terbutaline which does appear to have a significant effect to increase HR. The increased risk for first yr CAV development in AD pts requires further investigation.
CITATION INFORMATION: Kransdorf E, Kittleson M, Patel J, Aintablian T, Levine R, Kearney B, Musto N, Hage A, Geft D, Czer L, Esmailian F, Trento A, Kobashigawa J. Risk of Amiodarone and Permanent Pacemaker Placement After Heart Transplantation. Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Kransdorf E, Kittleson M, Patel J, Aintablian T, Levine R, Kearney B, Musto N, Hage A, Geft D, Czer L, Esmailian F, Trento A, Kobashigawa J. Risk of Amiodarone and Permanent Pacemaker Placement After Heart Transplantation. [abstract]. Am J Transplant. 2017; 17 (suppl 3). https://atcmeetingabstracts.com/abstract/risk-of-amiodarone-and-permanent-pacemaker-placement-after-heart-transplantation/. Accessed April 7, 2026.« Back to 2017 American Transplant Congress