Racial Equity in Living Donor Kidney Transplant: Center Variation and Opportunities for Progress
Duke University, Durham, NC
Meeting: 2022 American Transplant Congress
Abstract number: 512
Keywords: African-American, Living donor, Multivariate analysis, Surgery
Topic: Clinical Science » Kidney » 50 - Health Equity and Access
Session Information
Session Name: Health Equity and Access II
Session Type: Rapid Fire Oral Abstract
Date: Tuesday, June 7, 2022
Session Time: 5:30pm-7:00pm
 Presentation Time: 6:10pm-6:20pm
Presentation Time: 6:10pm-6:20pm
Location: Hynes Ballroom C
*Purpose: To estimate racial differences in living donor kidney transplant (LDKT) rates relative to patient, center and regional characteristics that may influence access to transplant.
*Methods: Retrospective cohort study of 88 US transplant centers that performed at least 12 LDKTs each year from 2008-2018 using USRDS and SRTR data. We calculated black/white LDKT rate ratios for each center-year, where a rate ratio of 1 indicates racial equity. Patient-level covariates were aggregated by center-year and calculated as percent of all waitlisted patients (type B blood, gender, post-secondary education, and cPRA >0.7). Modifiable center-level covariates that may increase LDKT were participation in the National Kidney Foundation Voucher Program, participation in the UNOS Paired Exchange Program, state Medicaid expansion and LDKT as a percent of kidney transplant volume. Regional characteristics were aggregated by transplant referral region (TRR) and included median percent uninsured, median prevalence of blacks, inter-quintile range of the area deprivation index and number of centers within the TRR. A generalized linear mixed model using Poisson likelihood was developed using fixed effects with by-race interactions for each covariate and random effects to enable correlation and variance to change over time.
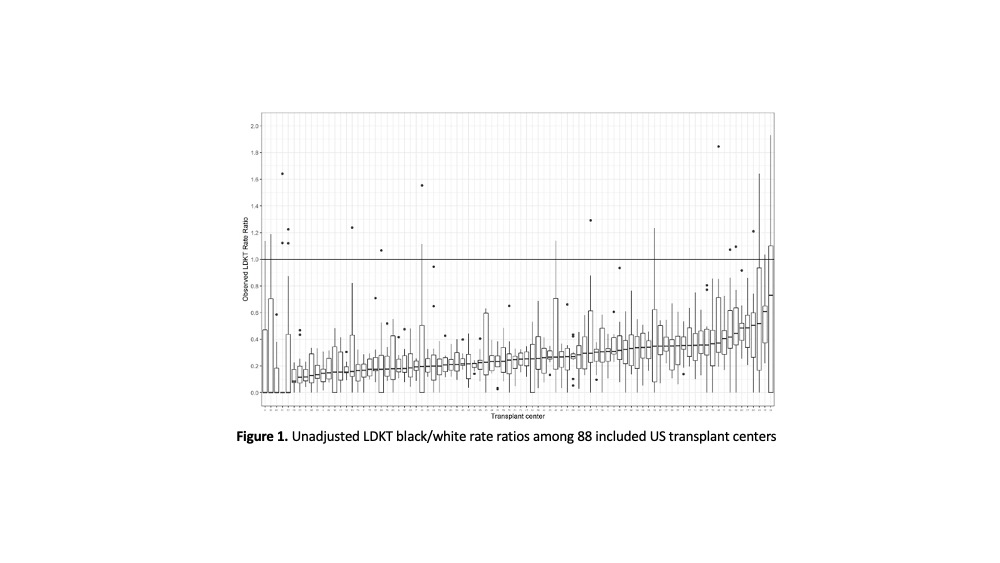
*Results: Among 88 centers over the 11-year study period, observed center-level black/white LDKT rate ratios ranged from 0 to 1.93 (Figure 1), with yearly medians ranging from 0.1968 to 0.3166. After adjusting for patient, center and regional characteristics, predicted center-level black/white LDKT rate ratios ranged from 0.0438 to 0.7702, with yearly medians ranging from 0.2197 to 0.2894. Adjusting modifiable center-level covariates to optimize center-level factors that may increase access to LDKT resulted in an increase in the minimum black/white rate ratio from 0.0438 to 0.0482 and an increase in the maximum rate ratio from 0.7702 to 0.8899. Relative to the observed 581 and 4401 LDKT in black and white patients, respectively, at the 88 included centers in 2018, the predicted increase in LDKT volume achieved by optimizing center-level modifiable covariates was 984 (69.4%) for black patients and 6734 (50.6%) for white patients.
*Conclusions: Despite several effective patient-level interventions, racial disparities in LDKT have persisted for more than 20 years. Transplant centers have a pivotal role in mitigating patient-level barriers and complementing patient-level interventions. Center-level interventions to improve equity in LDKT remain largely untested; this is a critical area for future research.
To cite this abstract in AMA style:
McElroy LM, Schappe T, Peskoe S, Wang V, Mohottige D, Scales CD, Pendergast J, Boulware L. Racial Equity in Living Donor Kidney Transplant: Center Variation and Opportunities for Progress [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/racial-equity-in-living-donor-kidney-transplant-center-variation-and-opportunities-for-progress/. Accessed April 4, 2026.« Back to 2022 American Transplant Congress