Is KDPI Valid for Hepatitis C Aviremic Kidneys?
1Surgery, University of Washington Medical Center, Seattle, WA
2Medicine, University of Washington Medical Center, Seattle, WA.
Meeting: 2018 American Transplant Congress
Abstract number: 29
Keywords: Kidney transplantation, Survival
Session Information
Session Name: Concurrent Session: Kidney Deceased Donor Allocation - 1
Session Type: Concurrent Session
Date: Sunday, June 3, 2018
Session Time: 2:30pm-4:00pm
 Presentation Time: 3:06pm-3:18pm
Presentation Time: 3:06pm-3:18pm
Location: Room 6E
KDRI is an estimate of post-transplant kidney graft failure. It is based on ten donor factors that independently affect transplant outcomes, including HCV status from serologic or NAT testing. With NAT now reported, further evaluation of these donors is now possible.
Methods: We conducted a retrospective matched case-control analysis of adult deceased donor kidney transplants performed between 12/5/2014 to 12/31/2016 obtained from UNOS databse. We identified kidney transplants that had both KDRI score and HCV Ab and NAT testing status. We compared 205 aviremic Hep C Ab+ NAT – kidney transplants to KDRI matched control kidneys that were Hep C Ab–NAT-.
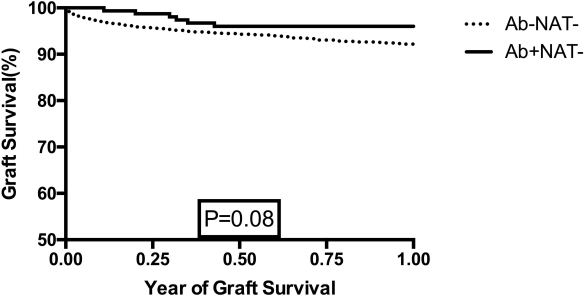
Results: The aviremic HCV kidneys were recovered from donors that were significantly younger 34.1±8.6 vs 42.6±10.4 years old, more likely to be white 183(89.3%) vs 1554(68.9%), less likely to have hypertension and diabetes. They were less likely to be DCD 13 vs 518 (P<0.0001). The majority of the recipients of the aviremic HCV kidneys when compared to match controls were Hepatitis C positive 90.2% vs 4.3%. The recipients were significantly older 59.5±7.4 vs 53.2±13.1 years old (P< 0.0001) and more likely to be male 162 (79%) vs 1378(61.1%) (P <0.0001). They were less likely to be white. They were more likely to be diabetic 105 (51.2%) vs 882(39.1%) (P=0.001).They were on dialysis for a shorter period of time 1175 ± 886 days vs 1949 ± 1311 days (P <0.0001) and were transplanted sooner 432 ± 556 vs 938.6 ±884 days (P <0.0001). The graft survival of aviremic HCV kidneys when compared to non-Hep C kidneys trended to be superior (Figure 1). If the HCV status of the aviremic kidneys were assumed to be negative, 122 more kidneys could have been allocated to patients with EPTS <20. Seven kidneys would no longer have KDPI>85%.
Conclusion: Further policies might consider these findings to appropriately allocate these kidneys to potentially extend graft survival and limit the organ discard rate.
Figure 1: HCV Ab+NAT- kidney allograft survival compared non-Hepatitis C kidneys Ab-NAT-
CITATION INFORMATION: Sibulesky L., Kling C., Blosser C., Johnson C., Limaye A., Bakthavatsalam R., Leca N., Perkins J. Is KDPI Valid for Hepatitis C Aviremic Kidneys? Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Sibulesky L, Kling C, Blosser C, Johnson C, Limaye A, Bakthavatsalam R, Leca N, Perkins J. Is KDPI Valid for Hepatitis C Aviremic Kidneys? [abstract]. https://atcmeetingabstracts.com/abstract/is-kdpi-valid-for-hepatitis-c-aviremic-kidneys/. Accessed March 29, 2026.« Back to 2018 American Transplant Congress