How Should Acute T-Cell Mediated Rejection of Kidney Transplants be Treated?
1University of Wisconsin, Madison, WI, 2University of Wisconsin, Verona, WI
Meeting: 2021 American Transplant Congress
Abstract number: 887
Keywords: Kidney transplantation, Outcome, Rejection
Topic: Clinical Science » Kidney » Kidney: Acute Cellular Rejection
Session Information
Session Name: Kidney: Acute Cellular Rejection
Session Type: Poster Abstract
Session Date & Time: None. Available on demand.
Location: Virtual
*Purpose: Many guidelines suggest treating acute T-cell mediated rejection (TCMR) of kidney allografts that is Banff grade I with steroids alone and Banff grade II with steroids plus anti-thymocyte globulin (ATG).
*Methods: We reviewed the kidney function and histological outcomes after treatment of 163 first episodes of biopsy-proven TCMR between 1/1/2015 and 07/31/2020. Patients with any component of antibody mediated rejection were excluded. Histological responses were defined: complete response (CR) as no residual rejection, partial response (PR) as improved Banff grade but persistent rejection, and no response (NR) as no change in Banff grade. Kidney function responses were defined: CR as eGFR returned to within 5ml/min/m2 of baseline eGFR, PR as improvement of eGFR by more than 5ml/min/m2 from nadir eGFR, and NR as eGFR staying above a value 5ml/min/m2 lower than peak eGFR.
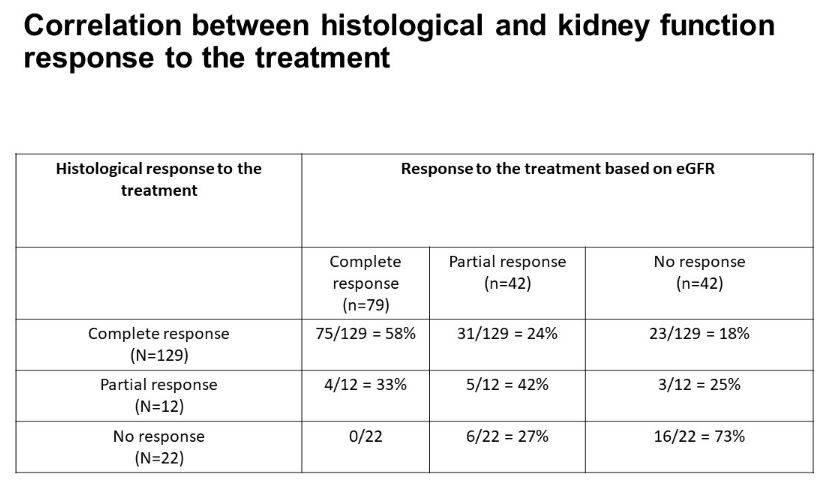
*Results: Of 163 kidney recipients with TCMR, 146 were treated with steroid pulse alone. 83% of patients with borderline rejection, 82.5% with grade 1A, 67% with grade 1B, and 50% with grade IIA had a histological CR or PR to treatment with steroids alone. Seventeen patients were treated with steroids plus ATG. The CR or PR response rate was 100% with grade 1A, 75% with grade 1B, 100% with grade IIA, and 57% with grade IIB. In patients with CR histologically, 58% had CR in their eGFR, but 18% had NR in eGFR. Of patients with PR histologically, 33% had CR, 42% had PR and 25% had NR based on eGFR. Of the 34 patients without CR histologically on the first biopsy who underwent additional treatment with steroids, 26 achieved CR. Histological and kidney function response to treatment was associated with better graft outcomes compared to patients with PR or NR to treatment (p=0.03 & 0.01 respectively). Multivariate analyses showed that higher grade of rejection was associated with worse long-term graft outcomes (HR=1.5, p=0.004, 95%Cl 1.13 to 1.99). Histological response and kidney function response to treatment was associated with improved graft outcomes (HR=0.64, p=0.04, 95%Cl 0.3961 to 1.0541; HR=0.5, p=0.003, 95%Cl 0.315 to 0.84 respectively).
*Conclusions: We demonstrate that responses based on kidney function alone do not correlate well with histological responses. Some patients with CR in eGFR have only PR histologically, and benefit from additional treatment. Others with NR in eGFR have CR histologically, and do not require additional treatment. These findings support the utility of protocol follow-up biopsies after treatment for TCMR to guide further treatment.
To cite this abstract in AMA style:
Aziz F, Parajuli S, Garg N, Mohamed M, Djamali A, Mandelbrot D. How Should Acute T-Cell Mediated Rejection of Kidney Transplants be Treated? [abstract]. Am J Transplant. 2021; 21 (suppl 3). https://atcmeetingabstracts.com/abstract/how-should-acute-t-cell-mediated-rejection-of-kidney-transplants-be-treated/. Accessed May 25, 2026.« Back to 2021 American Transplant Congress