High Prevalence of New Onset Diabetes Mellitus in a Predominantly Minority Urban Cohort of Kidney Transplant Recipients and Clinical Outcomes
Montefiore Medical Center, Albert Einstein College of Medicine, Bronx.
Meeting: 2018 American Transplant Congress
Abstract number: A219
Keywords: Kidney transplantation
Session Information
Session Name: Poster Session A: Kidney: Cardiovascular and Metabolic
Session Type: Poster Session
Date: Saturday, June 2, 2018
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Hall 4EF
Background: We aimed to determine the prevalence of new onset diabetes after transplant (NODAT) and its association with clinical outcomes in a cohort of predominantly Hispanic and Non-Hispanic Black kidney transplant recipients.
Methods: We performed a retrospective chart review of all recipients of kidney transplant from June 01, 2012 until December 31, 2014. Recipients with type 1 diabetes and those who received pancreas transplant were excluded. NODAT was defined by a hemoglobin A1c (A1c) 6.5% or higher, two random blood glucose levels of 200mg/dL or higher, or the use of glucose-lowering medication at any time after the transplant.
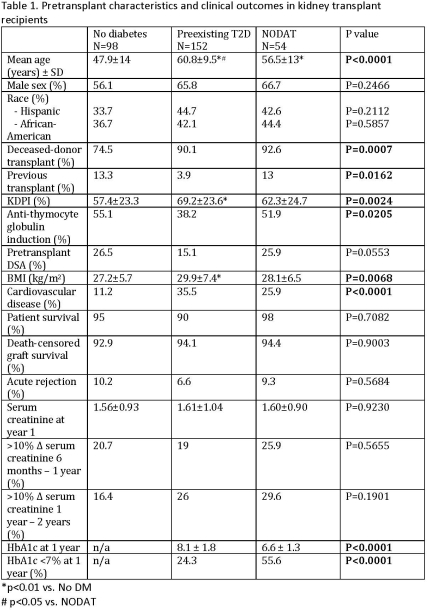
Results : A total of 304 individuals were included, 40% Hispanic and 41% non-Hispanic black. 152 recipients (50%) had pretransplant T2D. During a median follow up of 37 (22-52) months, 36% of the recipients without diabetes developed NODAT. Individuals with NODAT and T2D, compared to individuals without diabetes were older, had higher BMI, higher frequency of pretransplant cardiovascular disease, and received more deceased-donor grafts with higher KDPI scores. There was no significant difference between the groups in patient survival, graft survival, acute rejection rate, serum creatinine levels at one year post-transplant, and change in serum creatinine levels in the first two years. Recipients with NODAT, compared with T2D, had lower A1c (6.6±1.3% vs. 8.1±1.8%) and more frequently reached goal A1c of <7% (55.6% vs. 24.3%) at one year post transplant. Most frequent treatment for NODAT was diet only (42.6%), with 20.4% receiving DPP4 inhibitors, 20.4% metformin, 16.7% insulin, and 14.8% and sulfonylurea.
Conclusions: More than one third of recipients without diabetes at baseline developed NODAT. NODAT was not associated with inferior patient or graft survival or allograft function over the course of our relatively short follow up. While glycemic control in recipients with NODAT was better than in those with T2D, a significant proportion failed to reach the goal A1c , suggesting the need for earlier and better glycemic management.
CITATION INFORMATION: Aleksic S., Zahedpour S., Tsomos E., Ajaimy M., Zonszein J., Akalin E. High Prevalence of New Onset Diabetes Mellitus in a Predominantly Minority Urban Cohort of Kidney Transplant Recipients and Clinical Outcomes Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Aleksic S, Zahedpour S, Tsomos E, Ajaimy M, Zonszein J, Akalin E. High Prevalence of New Onset Diabetes Mellitus in a Predominantly Minority Urban Cohort of Kidney Transplant Recipients and Clinical Outcomes [abstract]. https://atcmeetingabstracts.com/abstract/high-prevalence-of-new-onset-diabetes-mellitus-in-a-predominantly-minority-urban-cohort-of-kidney-transplant-recipients-and-clinical-outcomes/. Accessed March 31, 2026.« Back to 2018 American Transplant Congress