De Novo Lipoprotein-X Causing Hypercholesterolemia and Acute Kidney Injury (AKI) in Simultaneous Liver Kidney Transplant (SLKT) Patient
Mayo Clinic, Phoenix, AZ
Meeting: 2022 American Transplant Congress
Abstract number: 1075
Keywords: Hypercholesterolemia, Kidney/liver transplantation, Lipoproteins, Renal function
Topic: Clinical Science » Liver » 52 - Liver: Kidney Issues in Liver Transplantation
Session Information
Session Name: Liver: Kidney Issues in Liver Transplantation
Session Type: Poster Abstract
Date: Sunday, June 5, 2022
Session Time: 7:00pm-8:00pm
 Presentation Time: 7:00pm-8:00pm
Presentation Time: 7:00pm-8:00pm
Location: Hynes Halls C & D
*Purpose: Cholestasis can cause reflux and spillage of biliary lipid into the plasma which can combine with albumin forming lipoprotein-X. Severe hypercholesterolemia mediated by lipoprotein-X has been described mainly in allogeneic bone marrow transplant due to chronic graft versus host disease of the liver. The incidence of such occurrence in liver transplantation is relatively uncommon.
*Methods: We describe a 37-year-old Caucasian female with a history of alcohol related cirrhosis and end stage renal disease from hepatorenal syndrome received a SLKT from a deceased after cardiac death donor on 2/2021.
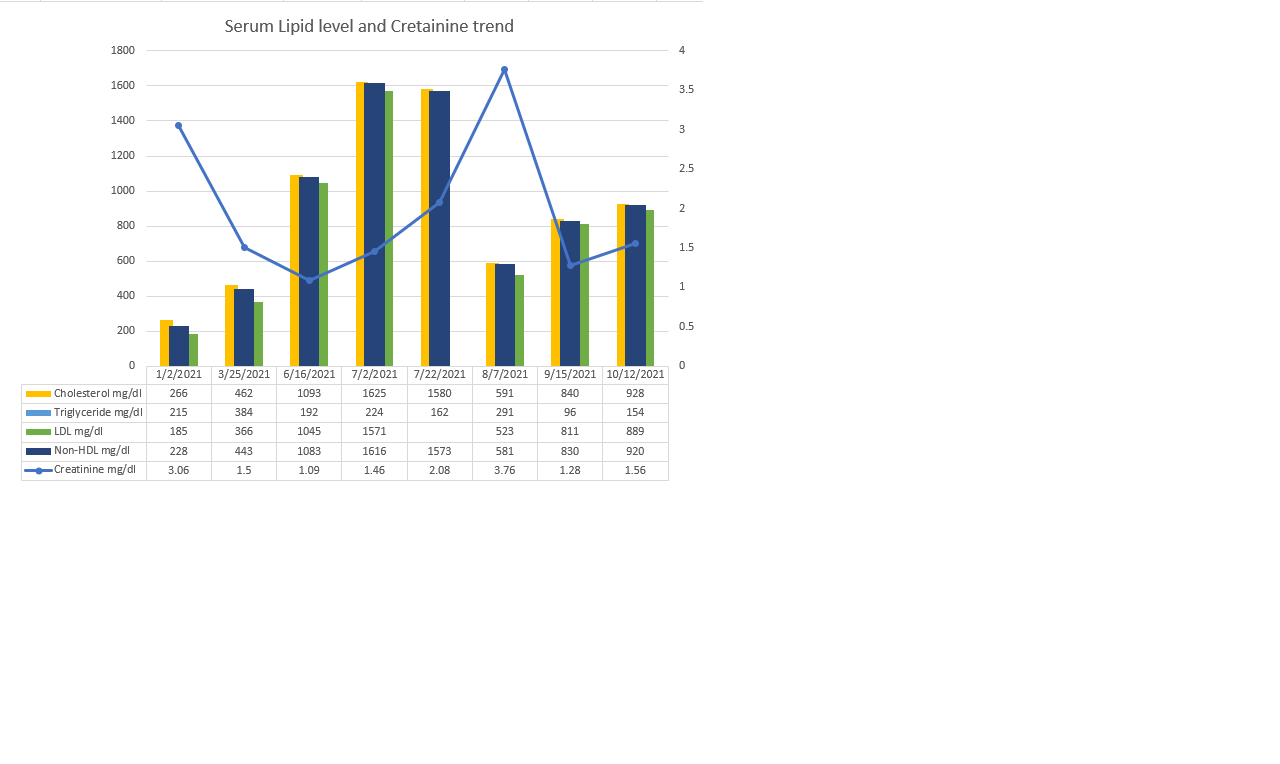
*Results: Donor liver biopsy showed minimal steatosis less than 5%. Her course was complicated by ischemic cholangiopathy with hepatolithiasis causing intrahepatic biliary obstruction requiring multiple endoscopic stents. Later, she developed pseudohyponatremia with sodium level of 126 mmol/L and serum osmolality of 308 mOsm/kg. It was related to hypercholesterolemia with total cholesterol of 1625 mg/dl and low-density lipoprotein (LDL) of 1571 mg/dl. Her serum creatinine increased from 0.8 mg/dl to 1.46 mg/dl. Renal allograft biopsy showed scattered oxalate crystals without rejection. Her serum oxalate level was high at 14.3 mcmol/L and urinalysis showing oxalate crystals. The decreased bile acid excretion may have enhanced net absorption of oxalate. She required dialysis briefly and was treated with high-intensity statins, ezetimibe, PCSK9 inhibitors and underwent lipid apheresis. She had positive lipoprotein-X and apolipoprotein B at 46mg/dl. Familial hypercholesterolemia genetic panel was negative and donor blood results showed normal liver function test, lipase, amylase and creatinine level. Her lipid profile and kidney allograft function subsequently improved after multiple sessions of lipid apheresis.
*Conclusions: Lipoprotein-X should be considered in pseudohyponatremia due to hypercholesterolemia associated cholestasis even in liver transplant recipients for early detection and treatment to prevent significant complications.

To cite this abstract in AMA style:
Me H, Nair SS, Al-Qaisi M, Ryan M, Kodali L, Aqel B. De Novo Lipoprotein-X Causing Hypercholesterolemia and Acute Kidney Injury (AKI) in Simultaneous Liver Kidney Transplant (SLKT) Patient [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/de-novo-lipoprotein-x-causing-hypercholesterolemia-and-acute-kidney-injury-aki-in-simultaneous-liver-kidney-transplant-slkt-patient/. Accessed March 24, 2026.« Back to 2022 American Transplant Congress