Center Effects Substantially Explain Disparities in Access to Kidney Transplants, Yet DSA Effects Remain
United Network for Organ Sharing, Richmond, VA
Meeting: 2020 American Transplant Congress
Abstract number: 487
Keywords: Allocation, Kidney transplantation, Waiting lists
Session Information
Session Name: All Organs: Disparities to Outcome and Access to Healthcare II
Session Type: Oral Abstract Session
Date: Saturday, May 30, 2020
Session Time: 3:15pm-4:45pm
 Presentation Time: 3:51pm-4:03pm
Presentation Time: 3:51pm-4:03pm
Location: Virtual
*Purpose: The OPTN developed a novel methodology in 2016 to monitor equity in access to deceased donor kidney transplants (Tx) among waitlisted candidates. Results have consistently shown donor service area (DSA) of listing to be the factor most independently associated with disparities. To better reflect disparities faced by WL candidates, the methodology is being expanded to incorporate center effects and parse out center- from DSA-level variation.
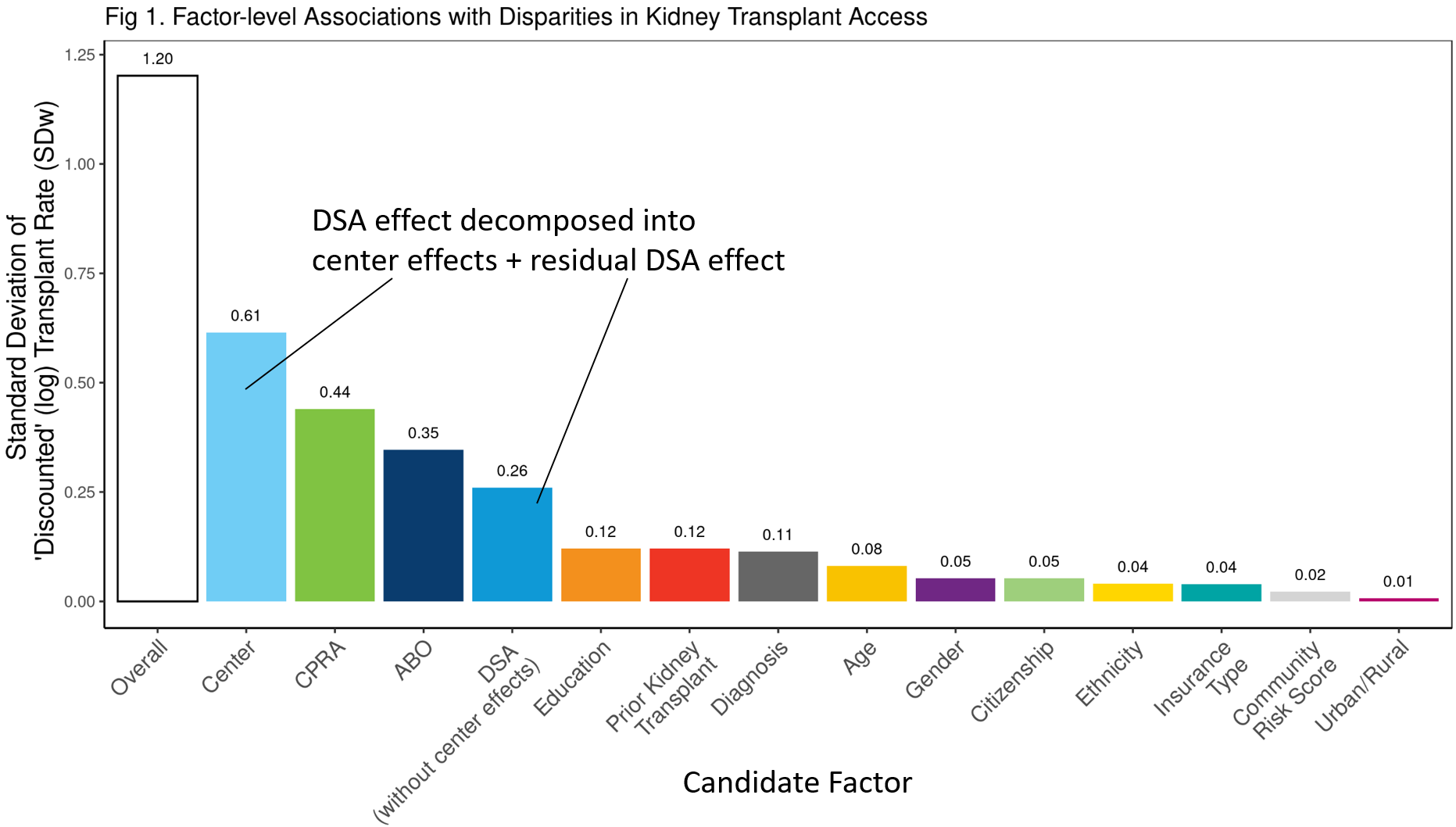
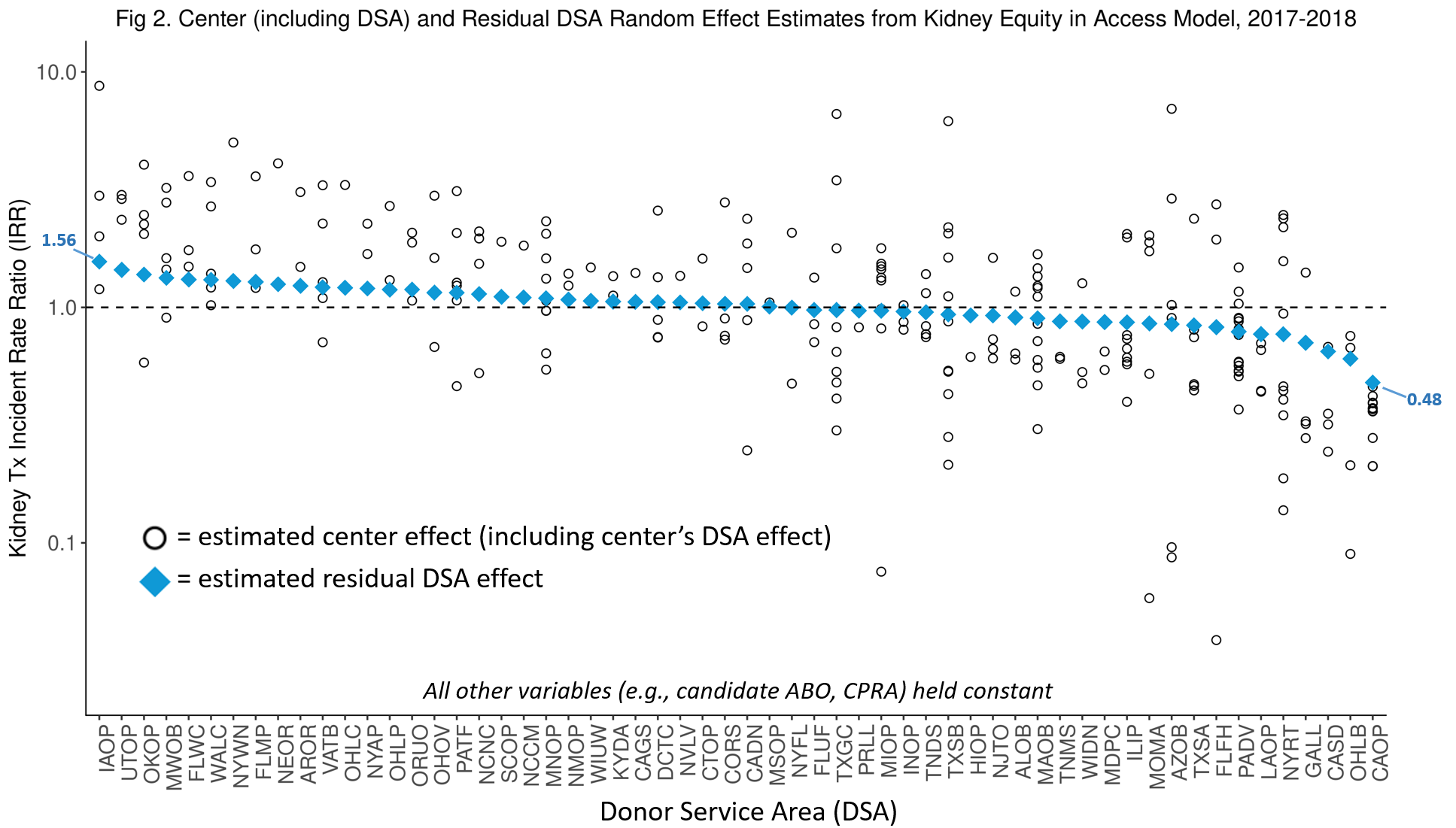
*Methods: Poisson tx rate regression with 17 candidate factors, including random DSA and nested center effects, was applied to a period-prevalent cohort (2017-2018) of active KI waiting list (WL) registrations using OPTN data. Overall disparity was quantified as the Winsorized standard deviation (SDw) of log(Tx rate) among registrations, after “discounting” for intentional variation (e.g., waiting time, ped priority) by holding such factors constant. To isolate each factor’s association with disparities, factor-specific SDw’s were obtained after holding all other factors constant. Random DSA and center Empirical Bayes (“shrunken”) estimates were expressed as Tx incidence rate ratios (IRRs).
*Results: Adding center effects increased the overall disparity metric 11% (SDw 1.08->1.20). Tx center was found to be the factor most associated with disparities in access (SDw=0.61). After removing center effects, substantial DSA effects remained (SDw=0.26), though DSA fell to 4th behind CPRA and ABO (Fig 1).
The open circles in Fig 2 result from combining each center’s effect with their DSA-specific effect. Centers in DSAs with above average IRR tended to have above average IRR, and vice versa. However, substantial heterogeneity in center-level IRRs was found even within the same DSA. After parsing out center effects, DSA IRRs ranged from 0.48 to 1.56, a 3.25-fold difference in Tx access (Fig 2).
*Conclusions: Tx center was found to be the top driver of kidney access disparities. But even after extracting center effects, substantial DSA disparities remain. Geographic disparities in access to transplant can be mitigated both via allocation policy changes (e.g., removing “local” (DSA) priority and distributing broadly to patients in need) and reducing center-level variation in organ utilization.
To cite this abstract in AMA style:
Stewart D, Robinson A, Klassen D, Wilk A. Center Effects Substantially Explain Disparities in Access to Kidney Transplants, Yet DSA Effects Remain [abstract]. Am J Transplant. 2020; 20 (suppl 3). https://atcmeetingabstracts.com/abstract/center-effects-substantially-explain-disparities-in-access-to-kidney-transplants-yet-dsa-effects-remain/. Accessed April 7, 2026.« Back to 2020 American Transplant Congress