Blood Pressure Evaluation by Three Different Modalities in Living Kidney Donors
Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH.
Meeting: 2015 American Transplant Congress
Abstract number: B171
Keywords: Donation, Hypertension, Kidney transplantation, Screening
Session Information
Session Name: Poster Session B: Living Donor Issues 1
Session Type: Poster Session
Date: Sunday, May 3, 2015
Session Time: 5:30pm-6:30pm
 Presentation Time: 5:30pm-6:30pm
Presentation Time: 5:30pm-6:30pm
Location: Exhibit Hall E
Screening for hypertension (HTN) is an important element of the living kidney donor (LKD) evaluation process. Since there are no general consensus about the blood pressure (BP) methodology to use in LKD, we sought to study how various BP modalities perform.
We studied 274 prospective LKD who had BP measured by the following modalities at time of evaluation: in-office BP (single BP using aneroid sphygmomanometer in the clinic), BpTRU BP (average of 5 automated readings in clinic using BpTRU device), and 24-hour ambulatory blood pressure monitoring (24-h ABPM), which is considered the gold-standard. HTN was defined following JNC8 guidelines. For each method we calculated the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV).
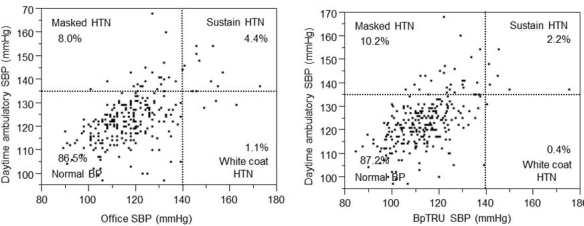
Donor age was 45±11 yo, 44% were male and 11% African American. Overall, 87.6% of screened donors were normotensive and 12.4% were hypertensive by 24-hr ABPM. Using office BP readings, 86.5%, 8%, 4.4% and 1.1% of LKD had normal BP, masked HTN, sustained HTN and white coat HTN respectively. When compared to 24h-ABPM, the sensitivity and specificity of office BP to diagnose HTN was 35% and 98.7% respectively, and the PPV and NPV were 80% and 91.5%, respectively. Using the BpTRU methodology, 87.2%, 10.2%, 2.2% and 0.4% of LKD had normal BP, masked HTN, sustained HTN and white coat HTN respectively. The sensitivity and specificity were 17.6% and 99.5% respectively, and the PPV and NPV were 85.7% and 89.5% respectively.
In conclusion, approximately 10% of prospective LKD have masked HTN and require the use of 24-hour ABPM for diagnosis. The BpTRU method does not add any advantage to the office single BP measurement, in part because white-coat HTN was uncommon in this population. Consideration should be given to the use of 24-hr ABPM despite the higher cost of the method especially in high risk populations.
To cite this abstract in AMA style:
Zaky Z, Thomas G, Gebreselassie S, Poggio E. Blood Pressure Evaluation by Three Different Modalities in Living Kidney Donors [abstract]. Am J Transplant. 2015; 15 (suppl 3). https://atcmeetingabstracts.com/abstract/blood-pressure-evaluation-by-three-different-modalities-in-living-kidney-donors/. Accessed March 28, 2026.« Back to 2015 American Transplant Congress