Acute Dialysis, Mortality and Renal Failure After Heart Alone Transplant by Egfr and Dialysis Requirement in the United States
1Medicine, University of Minnesota, Minneapolis, MN, 2Complex Care Analytics, Fairview Health Services, Minneapolis, MN, 3Surgery, University of Minnesota, Minneapolis, MN
Meeting: 2021 American Transplant Congress
Abstract number: 149
Keywords: Allocation, Heart transplant patients, Outcome
Topic: Clinical Science » Heart » Heart and VADs: All Topics
Session Information
Session Name: Do's and Don'ts of Heart Transplant Care
Session Type: Rapid Fire Oral Abstract
Date: Sunday, June 6, 2021
Session Time: 4:30pm-5:30pm
 Presentation Time: 5:05pm-5:10pm
Presentation Time: 5:05pm-5:10pm
Location: Virtual
*Purpose: We examined the early acute dialysis, 90-day mortality and one-year ESRD among OHT recipients by eGFR and dialysis requirement before transplantation.
*Methods: Utilizing the SRTR file, we identified all adult primary heart transplant recipients with eGFR less than 30 mL/min between 2000 and 2018. Recipients were categorized into 2 groups based on eGFR < 15 mL/min (n=127) and between 15-30 mL/min (n=901). Pre-transplant variables and post-transplant outcomes not subject to censoring were compared between the study groups using chi-square or Wilcoxon tests. For multivariable analysis, the outcomes of acute dialysis, 90-day mortality and one-year ESRD were analyzed using a generalized linear mixed model with transplant center as a random effect. Models were adjusted for age, gender, transplant indication, pre-transplant dialysis, last waitlist status and time on the waiting list.
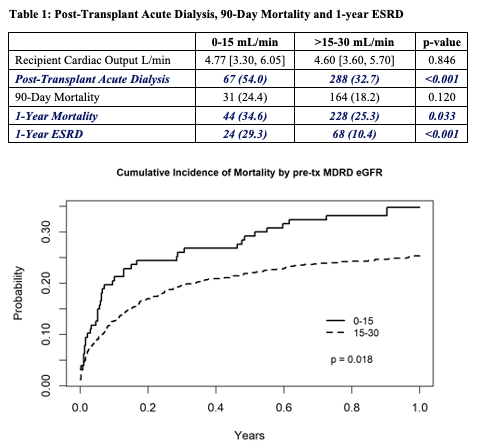
*Results: Acute dialysis post-transplant was more frequently observed in recipients with eGFR < 15 mL/min as compared to recipients with eGFR> 15 mL/min (54% vs. 32.7%, p<0.001). 90-day mortality was observed in 24.9 % of the lower eGFR group and 18.2% of the other group. Overall, the cumulative risk of mortality was higher in the lower eGFR group (Figure 1). The prevalence of renal failure among the surviving recipients was higher in recipients with eGFR< 15 mL/min as compared to those with > 15 -30 mL/min (29.3 % vs. 10.2%, p < 0.001). In the multivariable model, dialysis requirement before heart transplant alone was a strong predictor of acute dialysis, 90-day mortality and 1-year ESRD. Compared to recipients with eGFR< 15 mL/min, those with eGFR > 15-30 mL/min had lower risks of needing acute dialysis and 1-year ESRD. Recipients with congenital heart disease had a 2.6-fold increased risk of 90-day mortality than recipients with non-ischemic transplant indications.
*Conclusions: Owing to the high mortality of 35% at one year, heart transplant alone does not appear to be a viable option for those with low eGFR (<15 mL/min) or requiring dialysis. In comparison, the 15-30 mL/min group had lower mortality, approaching that of the Heart-Kidney transplant, and of those who survived, the majority 90% remained free of dialysis at one year. Perhaps, heart transplant alone with a safety net (either with advanced LD or DD) should be considered in this group. Our results are limited by the lack of data on renal failure acuity, which will need to be addressed in the future.
To cite this abstract in AMA style:
Aljuhani M, Alexy T, Jackson S, Martin C, Kandaswamy R, Riad S. Acute Dialysis, Mortality and Renal Failure After Heart Alone Transplant by Egfr and Dialysis Requirement in the United States [abstract]. Am J Transplant. 2021; 21 (suppl 3). https://atcmeetingabstracts.com/abstract/acute-dialysis-mortality-and-renal-failure-after-heart-alone-transplant-by-egfr-and-dialysis-requirement-in-the-united-states/. Accessed April 1, 2026.« Back to 2021 American Transplant Congress