Accepting Rejection in Liver Transplant Recipients Requiring Renal Replacement Therapy: A Practice Paradigm
1Pharmacy, University of Maryland Medical Center, Baltimore, MD, 2Nephrology, University of Maryland Medical Center, Baltimore, MD, 3Hepatology, University of Maryland Medical Center, Baltimore, MD, 4Transplant Surgery, University of Chicago Medical Center, Chicago, IL, 5Transplant Surgery, University of Maryland Medical Center, Baltimore, MD
Meeting: 2022 American Transplant Congress
Abstract number: 1074
Keywords: Immunosuppression, Infection, Rejection, Renal dysfunction
Topic: Clinical Science » Liver » 52 - Liver: Kidney Issues in Liver Transplantation
Session Information
Session Name: Liver: Kidney Issues in Liver Transplantation
Session Type: Poster Abstract
Date: Sunday, June 5, 2022
Session Time: 7:00pm-8:00pm
 Presentation Time: 7:00pm-8:00pm
Presentation Time: 7:00pm-8:00pm
Location: Hynes Halls C & D
*Purpose: The purpose of this study is to evaluate rejection outcomes in those requiring renal replacement therapy (RRT) after liver transplant.
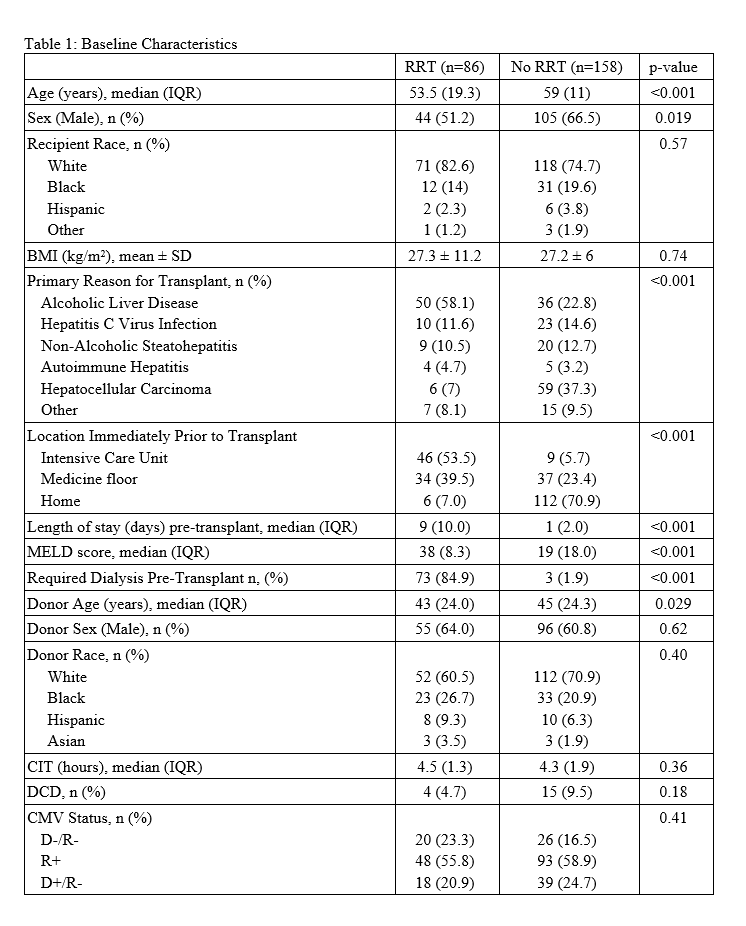
*Methods: This was a single center, retrospective, cohort study evaluating rejection in patients requiring RRT (n=86) vs. no RRT (n=158) that were transplanted between January 2017 and August 2019. The primary outcome was the incidence of biopsy proven acute rejection (BPAR) within 12-months. Secondary outcomes include patient and graft survival, infection, renal dysfunction, and immunosuppression practices within 12-months.
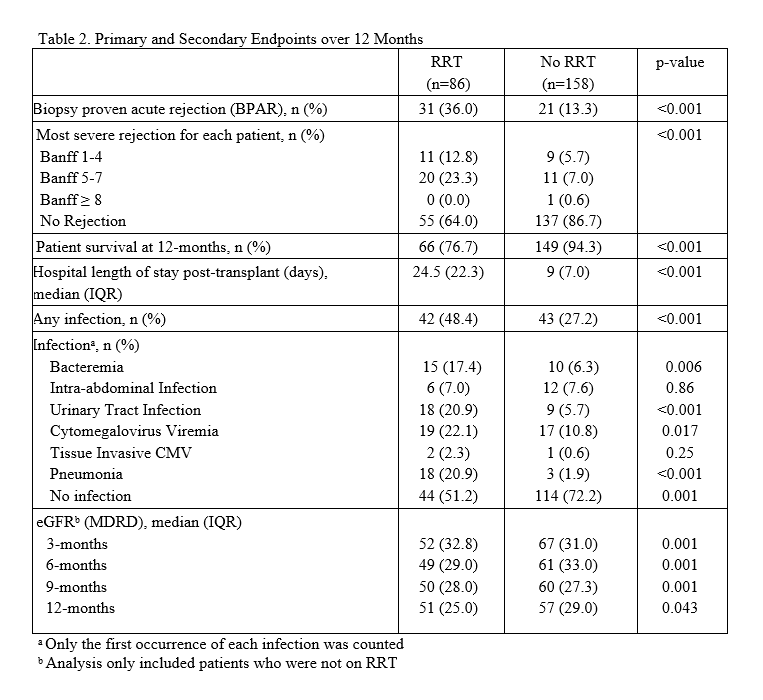
*Results: Differences in baseline characteristics (table 1) were not associated with increased rejection or mortality in a multivariable analysis. Median tacrolimus troughs were higher in the no RRT group at all time points except at 12-months (P=0.065). BPAR at 12-months post-transplant was significantly higher amongst those requiring RRT (36% vs. 13%, P<0.001). All rejections were mild to moderate in severity, with more treated rejections in the RRT group (13% vs. 4%, P=0.008). Patient survival at 12-months was 77% for those receiving RRT and 94% for those not requiring RRT (P<0.001) (table 2). Infection (HR 3.8, 95% CI 1.6-8.8; P<0.001), but not rejection (HR 0.7, 95% CI 0.3-1.7; P=0.5) was an independent predictor of mortality (table 3).
*Conclusions: Although the incidence of rejection was higher in those requiring RRT, our study suggests that permissive rejection may be an acceptable strategy in patients receiving RRT following liver transplant to balance the detrimental impact of infection on mortality.
To cite this abstract in AMA style:
Farghaly S, Sparkes T, Masters B, Haririan A, Jakhete N, Barth RN, Maluf D, Freedman S. Accepting Rejection in Liver Transplant Recipients Requiring Renal Replacement Therapy: A Practice Paradigm [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/accepting-rejection-in-liver-transplant-recipients-requiring-renal-replacement-therapy-a-practice-paradigm/. Accessed March 25, 2026.« Back to 2022 American Transplant Congress