Similar Outcomes Can Be Expected Among HIV (+) Kidney Transplant Recipients (HIV+ Tx) Vs. HIV (-) Kidney Transplant Recipients (HIV- Tx) Receiving Similar Immunosuppression Protocols
1Dept of Medicine, Drexel University College of Medicine, Philadelphia
2Dept of Surgery, Drexel University College of Medicine, Philadelphia
3Dept of Pharmacy, Hahnemann University Hospital, Philadelphia, PA.
Meeting: 2015 American Transplant Congress
Abstract number: A82
Keywords: HIV virus, Kidney transplantation, Outcome
Session Information
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Exhibit Hall E
Outcomes among HIV+ Tx continue to improve despite the established risk of rejection and calcineurin-nephrotoxicity. We sought to compare outcomes among HIV+ Tx vs. HIV- Tx receiving similar immunosuppression protocols.
Methods: Retrospective analysis of all HIV +/- Tx performed since 2011, receiving basiliximab + calcineurin inhibitor based immunosuppression. HIV+ Tx received IVIg as an additional induction agent. Clinical outcomes were assessed between the HIV+ Tx and HIV- Tx groups at 1 year post-transplant. All rejections were considered, including subclinical and borderline.
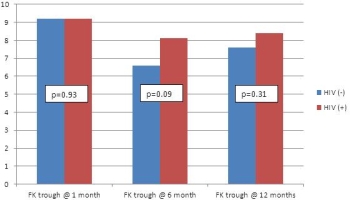
Results: In total, 39 patients were reviewed. Table 1 illustrates comparable recipient and donor characteristics. Donor age was younger among the HIV+ Tx, but KDRI was similar. Despite the potential for drug interactions among HIV+ Tx, tac troughs levels were comparable at all time points (Figure 1). Clinical post-Tx outcomes are comparable at all time points (Table 2). On follow-up biopsies, the incidence of mild fibrosis was more common among HIV + Tx (62% vs. 36%).
Conclusion: Immunosuppression protocols utilized among HIV- Tx can attain similar outcomes in HIV+ Tx. Standard markers of allograft function (i.e. eGFR) may not reflect degree of fibrosis on Biopsies in the HIV+ Tx. This may be reflected by the continuation of similar tac troughs throughout the post-Tx period..
| Table 1 | HIV (-) | HIV (+) | p-value |
| Recipient Age | 57 ± 14 | 51 ± 8 | 0.03 |
| African American | 32% | 54% | 0.16 |
| Male | 76% | 92% | 0.16 |
| HCV (+) | 16% | 8% | 0.50 |
| HD vintage (months) | 41 ± 40 | 81 ± 38 | 0.004 |
| Incidence of Delayed Graft Function | 28% | 46% | 0.23 |
| Deceased Donor | 80% | 92% | 0.93 |
| Donor age | 42 ± 13 | 30 ± 11 | 0.004 |
| KDRI score | 0.99 ± 0.26 | 0.94 ± 0.16 | 0.71 |
| Table 2 | HIV (-) | HIV (+) | p-value |
| Proteinuria @ 1 year | 0.18 ± 0.10 | 0.26 ± 0.23 | 0.73 |
| eGFR @ 1 year (mL/min) | 57 ± 18 | 58 ± 20 | 1.0 |
| Incidence of BK viremia @ 1 year | 24% | 8% | 0.28 |
| ACR | 24% | 38% | 0.67 |
To cite this abstract in AMA style:
Panarey L, Malat G, Sharma A, Ranganna K, Reich D, Xiao G, Doyle A. Similar Outcomes Can Be Expected Among HIV (+) Kidney Transplant Recipients (HIV+ Tx) Vs. HIV (-) Kidney Transplant Recipients (HIV- Tx) Receiving Similar Immunosuppression Protocols [abstract]. Am J Transplant. 2015; 15 (suppl 3). https://atcmeetingabstracts.com/abstract/similar-outcomes-can-be-expected-among-hiv-kidney-transplant-recipients-hiv-tx-vs-hiv-kidney-transplant-recipients-hiv-tx-receiving-similar-immunosuppression-protocols/. Accessed April 27, 2026.« Back to 2015 American Transplant Congress