Impact of Traveling for Transplant on Access to and Outcomes from Kidney and Liver Transplantation
1Emory University, Atlanta, GA, 2University of Iowa, Ames, IA
Meeting: 2021 American Transplant Congress
Abstract number: 701
Keywords: Outcome, Public policy
Topic: Clinical Science » Public Policy » Non-Organ Specific: Public Policy & Allocation
Session Information
Session Name: Non-Organ Specific: Public Policy & Allocation
Session Type: Poster Abstract
Session Date & Time: None. Available on demand.
Location: Virtual
*Purpose: Newly developed transplant referral regions (TRRs) can be used to understand how and why patients travel outside of their home transplant center to receive care. We used TRRs to estimate the association between travel for transplant and transplant access and outcomes for kidney and liver candidates.
*Methods: We obtained data on adult kidney and liver transplant candidates listed from 2006 to 2016 from SRTR. Traveling for transplant was defined using TRRs, and categorized as (1) no travel, (2) travel to a neighboring TRR, (3) travel to an outside TRR, or (4) dually listed in home TRR and outside TRR. We estimated cause-specific hazard ratios for the association between transplant travel, time to transplant, and waitlist mortality, adjusting for clinical and demographic factors. We used Cox proportional hazards models to estimate the association between transplant travel and post-transplant survival.
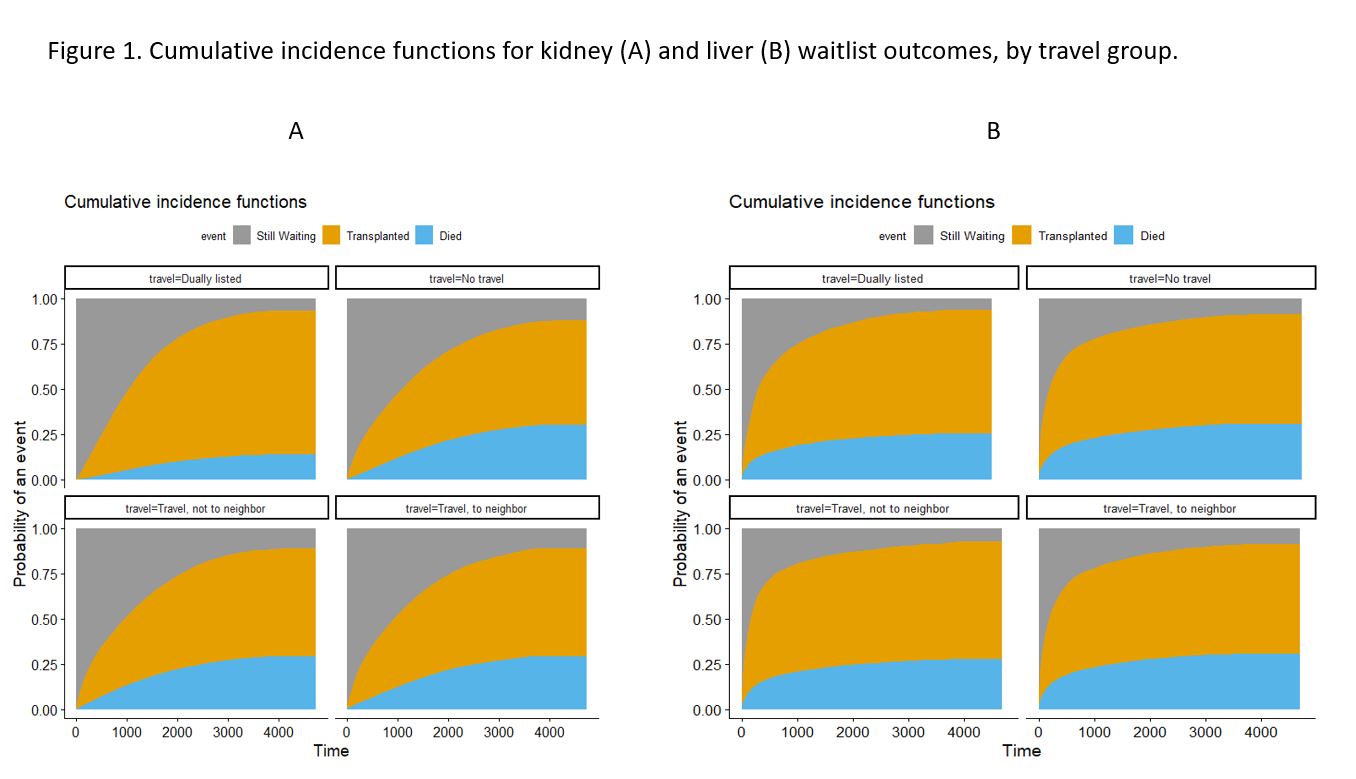
*Results: Between 2006 and 2016, 108,864 kidney and 32,314 liver candidates were listed outside their home TRR. Kidney candidates who traveled had higher transplant rates (Figure 1A). After adjustment, transplant rates were 7% higher for those who traveled to a neighbor, 12% higher for those who traveled to a non-neighbor, and 23.5% higher for dually listed patients compared to non-travelers. Those who traveled to a neighbor had 7% higher waitlist mortality (csHR: 1.07, 95% CI: 1.05, 1.10) than those who did not travel, while dually listed patients had nearly 50% lower waitlist mortality (csHR: 0.55, 95% CI: 0.53, 0.57). However, dually listed patients had higher post-transplant mortality than non-travelers (HR: 1.45, 95% CI: 1.38, 1.52). Among liver candidates, only those who traveled to a non-neighboring TRR had higher transplant rates relative to those who did not travel (Figure 1B, csHR 1.15, 95% CI: 1.13, 1.19). Dually listed candidates had lower waitlist mortality (csHR 0.80, 95% CI: 0.75, 0.85). Those who traveled to a non-neighboring TRR (HR: 1.06, 95% CI: 1.01, 1.12) and dually listed candidates (HR: 1.60, 95% CI: 1.10, 2.33) had higher post-transplant mortality than those who did not travel.
*Conclusions: Traveling for transplant was associated with higher rates of transplant and shorter waiting time, but dually listed candidates appeared to have higher post-transplant mortality. Further research is needed to understand how transplant travel affects patients, transplant centers, and the communities they serve.
To cite this abstract in AMA style:
Ross-Driscoll K, Lynch R, Axelrod D, Patzer R. Impact of Traveling for Transplant on Access to and Outcomes from Kidney and Liver Transplantation [abstract]. Am J Transplant. 2021; 21 (suppl 3). https://atcmeetingabstracts.com/abstract/impact-of-traveling-for-transplant-on-access-to-and-outcomes-from-kidney-and-liver-transplantation/. Accessed May 31, 2026.« Back to 2021 American Transplant Congress