Transplantation of Hepatitis C Virus Positive Donor Kidneys into Hepatitis C Negative Older Recipients
1Surgery, Montefiore Medical Center, Bronx, NY, 2Medicine, Montefiore Medical Center, Bronx, NY, 3Epidemiology and Psychiatry, Montefiore Medical Center, Bronx, NY, 4Medical Affairs, Montefiore Medical Center, Bronx, NY, 5Risk & Loss Prevention, Montefiore Medical Center, Bronx, NY, 6Pharmacy, Montefiore Medical Center, Bronx, NY
Meeting: 2019 American Transplant Congress
Abstract number: D358
Keywords: Donation, Hepatitis C, Kidney transplantation
Session Information
Session Name: Poster Session D: Late Breaking
Session Type: Poster Session
Date: Tuesday, June 4, 2019
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:00pm-7:00pm
Presentation Time: 6:00pm-7:00pm
Location: Hall C & D
*Purpose: Patients awaiting transplantation are often at risk of developing life-threatening disease and complications. Older patients have a disproportionately higher risk of dropping out of the waitlist due to their greater burden of co-morbidities and frailty. Acceptable donors are the main roadblock to increasing transplant rate in this patient population.
*Methods: Here we describe the utilization of HCV-infected kidneys (viral positive) transplanted into non-infected recipients (D+/R-) in older patients and compare them to a similar group. Informed consent was obtained on all patients. Anti-HCV treatment was started on post-operative day 8 (mean).
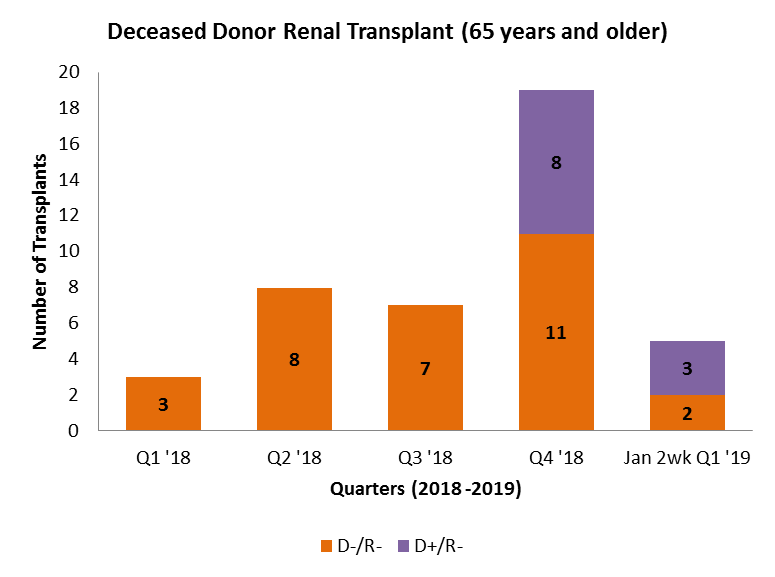
*Results: Eleven D+/R- transplants were performed in patients 65 years and older starting November 2018 at our center. Comparing this group to 65 years and older recipients (n=31) of non-infected donor kidneys (D-/R-) there is no difference in mean recipient age (71 v. 69; p=0.8). There was no difference between D+/R- and D-/R- in mean donor age (39 v. 44.8; p=0.3), KDPI (76 v. 67.6; p=0.13), donor terminal creatinine (1.8 mg/dL v. 2.5 mg/dL; p=0.28), cold ischemic time (1844 min v. 1770 min.; p=0.6). Negating HCV status for KDPI resulted in the D+/R- cohort having significantly lower values as compared to the D-/R- group (55 v. 67.6; p=0.04). As such, none of D+/R- patients have had delayed graft function (DGF), while DGF was evident in 58% of D-/R- recipients. Moreover, the D+/R- cohort seemed to leave the hospital sooner as compared to the D-/R- group (4 days v. 6.6 days; p=0.04). Lastly, D+/R- transplantation resulted in a quarterly upsurge in transplantation of our older recipients.[figure 1]
*Conclusions: Given the recent introduction of this policy, all D+/R- patients are currently receiving glecaprevir/pibrentasvir and treatment response assessment is underway. The net impact of this policy was to facilitate transplantation in our older patient population by allowing access to a historically unavailable donor pool. More research is needed to understand why D+/R- recipients have lower rates of DGF and leave the hospital much sooner. However, KDPI likely underestimates the performance of HCV-infected kidneys.
To cite this abstract in AMA style:
Graham JA, Ajaimy M, Torabi J, Powell T, Weiss J, Weinstein T, Greenstein S, Andacoglu O, Campbell A, Carrero J, Lapponese J, Kinkhabwala M, Akalin E, Rocca JP. Transplantation of Hepatitis C Virus Positive Donor Kidneys into Hepatitis C Negative Older Recipients [abstract]. Am J Transplant. 2019; 19 (suppl 3). https://atcmeetingabstracts.com/abstract/transplantation-of-hepatitis-c-virus-positive-donor-kidneys-into-hepatitis-c-negative-older-recipients/. Accessed May 19, 2026.« Back to 2019 American Transplant Congress