Contemporary Desensitization with Low Dose Rituximab Ensures Kidney Transplant Outcome beyond ABO Blood Type Incompatibility:A Comparison between past Regimens in Single Institute
Kidney Transplant Surgery and Urology, Sapporo City General Hospital, Sapporo, Japan.
Meeting: 2018 American Transplant Congress
Abstract number: A154
Keywords: Antibodies, Immunosuppression, Kidney transplantation, Plasmapheresis
Session Information
Session Name: Poster Session A: Kidney Immunosuppression: Desensitization
Session Type: Poster Session
Date: Saturday, June 2, 2018
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Hall 4EF
INTRODUCTION: An ABO incompatible kidney transplant (ABOiKT) requires desensitization (DS). The ways of DS have been changed chronologically and the outcome could have been subsequently improved. Here we compared the outcome of ABOiKT in our institute according to the types of regimens.
METHODS: 131 ABOiKT since 1994 to 2016 were enrolled. They were divided into 4 categories according to DS. In Era I (n=18), preoperative immunosuppressants (IS) comprising CSA/AZA/CS were administered on D-3. In Era II (n=7), IS (TAC/MMF/CS) were initiated from D-14 and basiliximab (BSX) was administered. In Era III (n=53), IS (TAC/MMF/CS/BSX) were administered as in Era II. In Era IV (n=53), everolimus (EVR) was added from the beginning of IS (TAC/MMF/CS/BSX) initiation and CS were discontinued on Day 4 in some cases. Simultaneous splenectomy was done in Era I and II. Recipients in Era II to IV accepted low dose rituximab (RIT) (50mg/m2 to 200mg/body). Plasmapheresis (PP) was performed from 2 to 4 sessions according to the strength of anti-blood type antibodies (ABA) in most of patients. However, patients whose initial ABA within 16x were encouraged to spare PP in Era IV.
RESULTS: 3 out of 131 patients lost their grafts within 2 weeks due to acute antibody mediated rejection (AMR) (2 in Era I, 1 in Era III). Another patient in Era I exhibited severe HUS caused by AMR and ceased the function. Interestingly, the positivity of complement deposition (C3 or C4d) of 1H graft biopsy was higher in Era I compared to that in Era II-IV (6/18 vs. 10/106, p=0.0131). More interestingly, the half of positive cases in Era I developed AMR but none in those in ERA II-IV. Graft survivals are improving Era by Era (p=0.0157). 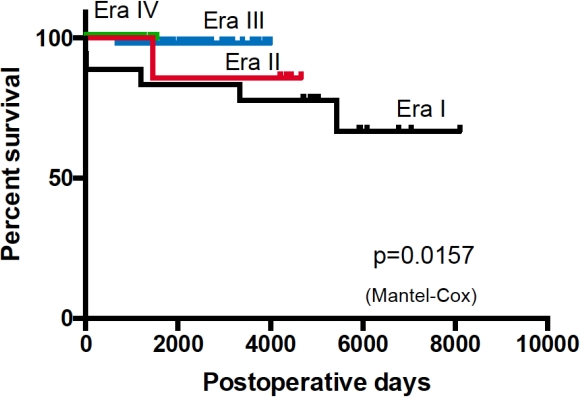
CONCLUSION: The outcome of contemporary ABOiKT using low dose RIT is excellent even without splenectomy with certain suppression of humoral immunity. Among them, additional RIT could bring equivalent or more excellent outcome without excessive PP in some cases. The longer follow-up should be warranted.
CITATION INFORMATION: Harada H., Wada Y., Mitsuke A., Hirose T., Fukuzawa N., Seki T. Contemporary Desensitization with Low Dose Rituximab Ensures Kidney Transplant Outcome beyond ABO Blood Type Incompatibility:A Comparison between past Regimens in Single Institute Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Harada H, Wada Y, Mitsuke A, Hirose T, Fukuzawa N, Seki T. Contemporary Desensitization with Low Dose Rituximab Ensures Kidney Transplant Outcome beyond ABO Blood Type Incompatibility:A Comparison between past Regimens in Single Institute [abstract]. https://atcmeetingabstracts.com/abstract/contemporary-desensitization-with-low-dose-rituximab-ensures-kidney-transplant-outcome-beyond-abo-blood-type-incompatibilitya-comparison-between-past-regimens-in-single-institute/. Accessed May 14, 2026.« Back to 2018 American Transplant Congress