Local Expansion in DCD Kidney Transplant Activity Improves Waiting List Outcomes and Addresses Inequities of Access to Transplantation
1Cambridge University, Cambridge, United Kingdom
2NHSBT, Bristol, United Kingdom.
Meeting: 2015 American Transplant Congress
Abstract number: C39
Keywords: Donors, Elderly patients, non-heart-beating, Resource utilization, Waiting lists
Session Information
Session Name: Poster Session C: ECD/DCD/high KDPI
Session Type: Poster Session
Date: Monday, May 4, 2015
Session Time: 5:30pm-6:30pm
 Presentation Time: 5:30pm-6:30pm
Presentation Time: 5:30pm-6:30pm
Location: Exhibit Hall E
Introduction: Following expansion in our circulatory death (DCD) transplant program, our center now performs twice as many DCD as brain-death (DBD) kidney transplants. Here, we investigate how a large pool of locally-allocated DCD kidneys influences outcomes for waiting list populations of different ages.
Methods: A retrospective observational cohort study comparing outcomes for adults listed for renal transplantation between 2002 and 2012 according to age at listing: under 45 (Grp A); 45 to 65 (Grp B); and over 65 (Grp C). DCD and DBD kidneys were allocated according to a similar algorithm, but as DCD kidneys were not shared nationally, additional constraints, typically recipient age, were applied in their allocation. Data on UK transplant activity was obtained from NHSBT and cross-referenced locally.
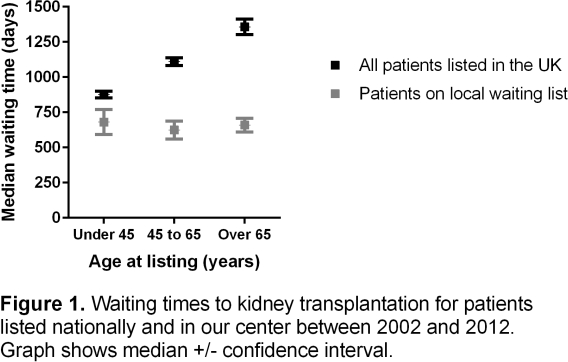
Results: Compared to UK data, listed patients of all ages in our center waited significantly less for a transplant. Consequently, overall transplantation rates were higher for our patients, and waiting-list deaths lower. This effect was most apparent for Grp C patients, whose median time to transplant was much shorter than the national average and notably, was comparable to waiting times for our Grp A and B patients (Fig 1).
Proportions of live donor, DBD and DCD kidneys were strikingly different between the recipient groups in our center, with Grp A patients receiving approximately equal proportions of each, whereas two-thirds of the kidneys transplanted to Grp C patients were from DCD donors (p<0.001). However, the majority of DCD kidneys were still transplanted to younger recipients (n=131, 244, 46 for Grps A to C, respectively), because far fewer elderly patients are listed. Transplantation was associated with a survival benefit from listing for Grps A and B but not C, where survival for listed and transplanted patients was similar.
Discussion: Local expansion in DCD kidney transplant activity improves survival outcomes from listing in younger patients and although not conferring a survival advantage for older patients, may address inequity of access to transplantation.
To cite this abstract in AMA style:
Mirshekar-Syahkal B, Bradbury L, Sun P, Aly M, Berry M, Norris J, Bradley J, Pettigrew G. Local Expansion in DCD Kidney Transplant Activity Improves Waiting List Outcomes and Addresses Inequities of Access to Transplantation [abstract]. Am J Transplant. 2015; 15 (suppl 3). https://atcmeetingabstracts.com/abstract/local-expansion-in-dcd-kidney-transplant-activity-improves-waiting-list-outcomes-and-addresses-inequities-of-access-to-transplantation/. Accessed May 1, 2026.« Back to 2015 American Transplant Congress